What are inequalities in mental health?
Mental health conditions are not distributed evenly across the population: some groups are a substantially higher risk of experiencing low wellbeing and mental health conditions. Much of these inequalities result from complex interactions of inequalities in wealth and power; including racism, misogyny, homophobia and other forms of injustice (Centre for Mental Health, 2020). It is important to consider how these relate to wider social and environmental determinants of health (as covered in Chapter One), such as poverty and income (Centre for Mental Health, 2020).
This report follows the CORE20PLUS5 approach to understanding healthcare inequalities (3). As such, the following groups have been identified as being at higher risk of mental health conditions:
- CORE20: the most deprived 20% of the population.
- PLUS populations: groups at risk of health inequalities and inclusion health groups.
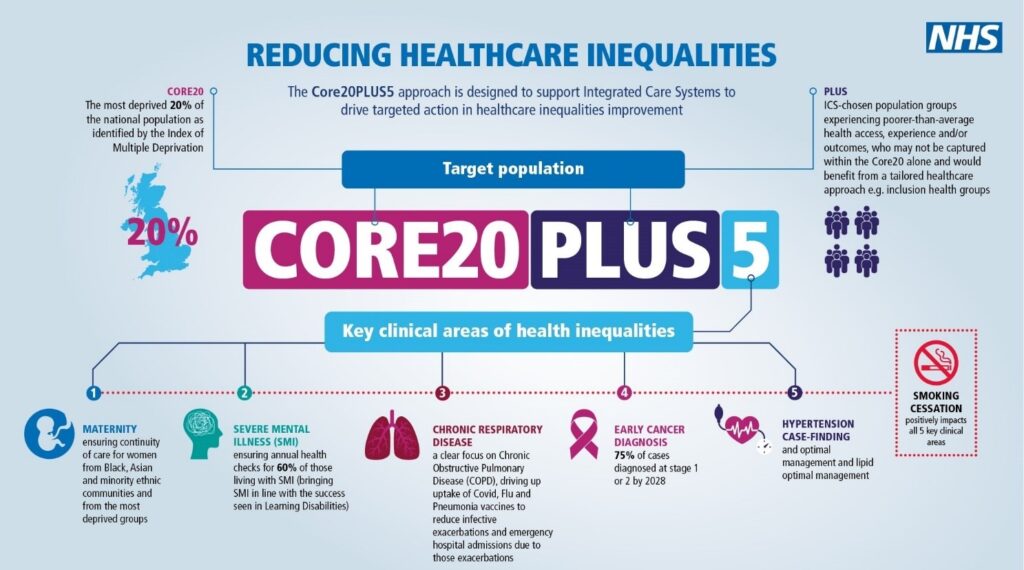
Figure 5: The CORE20PLUS5 approach to reducing health inequalities (note that there are also CORE20PLUS5 populations for children and young people). Source: NHS England
Inequalities in mental health services
Some groups face a ‘triple barrier’ of poorer access to appropriate mental health services, and worse experiences and outcomes when they are able to access support (Centre for Mental Health, 2020).
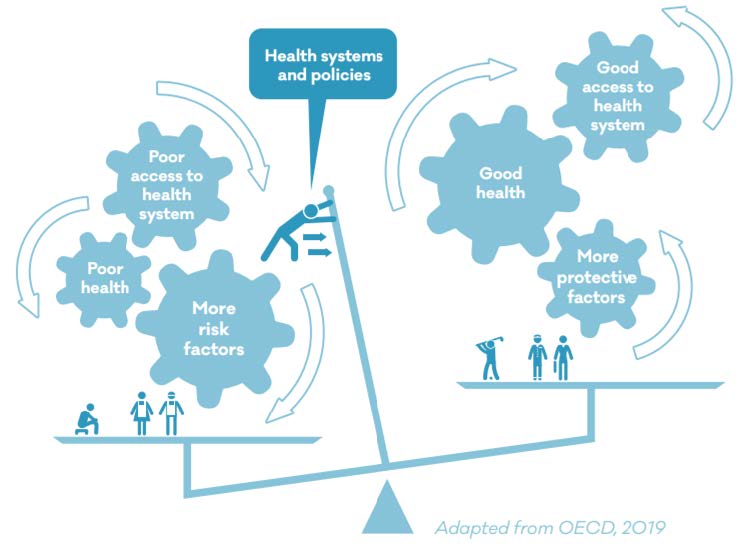
Figure 6: The perpetuation of health inequalities. Source: Mental Health Foundation
This subsection will explore:
- Inequalities in mental health in different population groups, in terms of the prevalence of mental health conditions and risk factors for poor mental health; and
- Mental health service inequalities, in terms of service users’ access, experiences and outcomes.
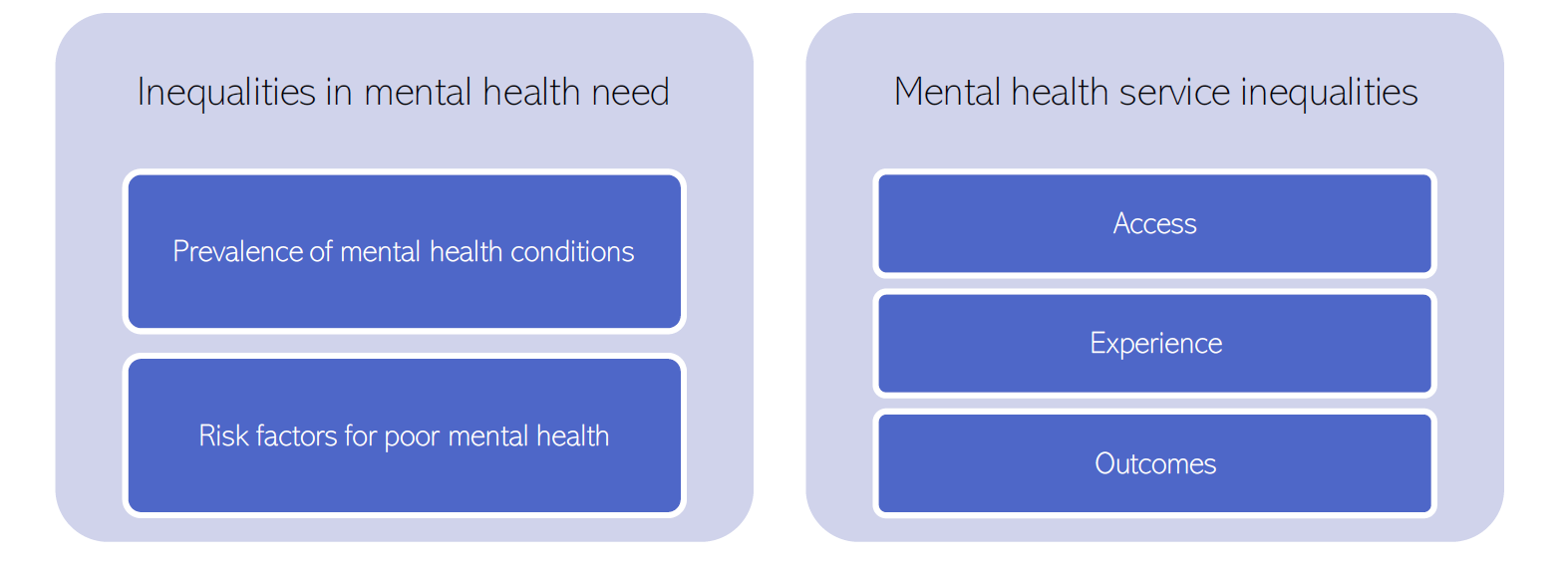
Figure 7: Layout of chapter sub-section
Understanding inequalities
It is important to understand inequalities from the perspectives of people who are most impacted. Designing solutions to these inequalities must stem from meaningful collaboration between healthcare services and local communities (Turakhia & Combs, 2017).
- An intersectional approach is needed to consider that people who experience multiple social injustices may face specific disadvantages, some of which can be reinforced due to the interactions.
- Use of healthcare services is not necessarily a reflection of equity of access: whether or not people access services depends is dependent on the interplay between people and their social contexts, as well as health services themselves (Dixon-Woods et al., 2006). This is known as candidacy theory.
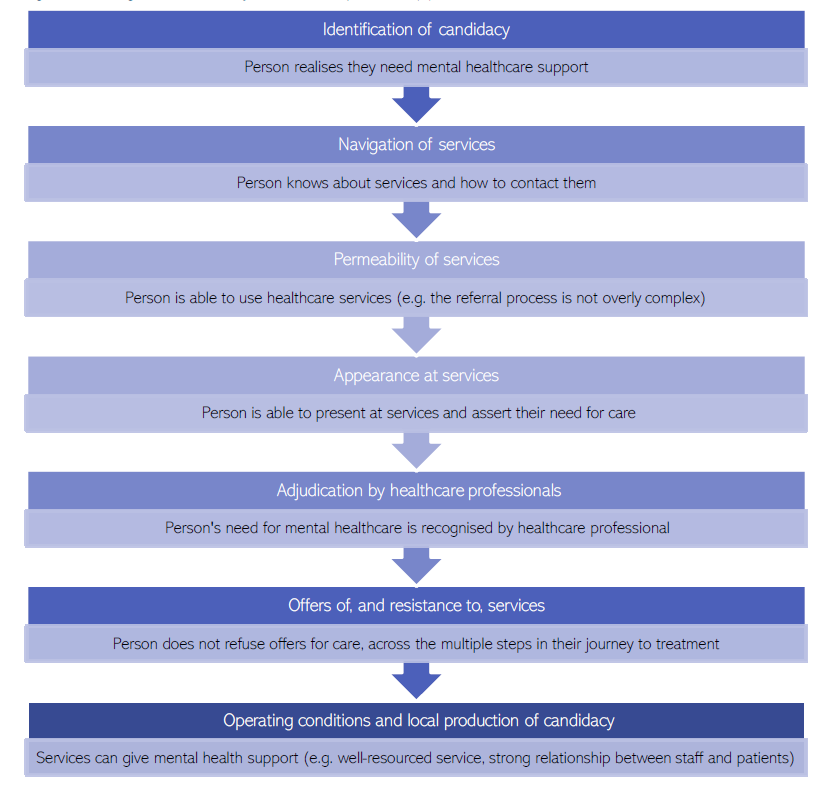
Figure 8: The stages of the candidacy framework. Adapted from: (Dixon-Woods et al., 2006)
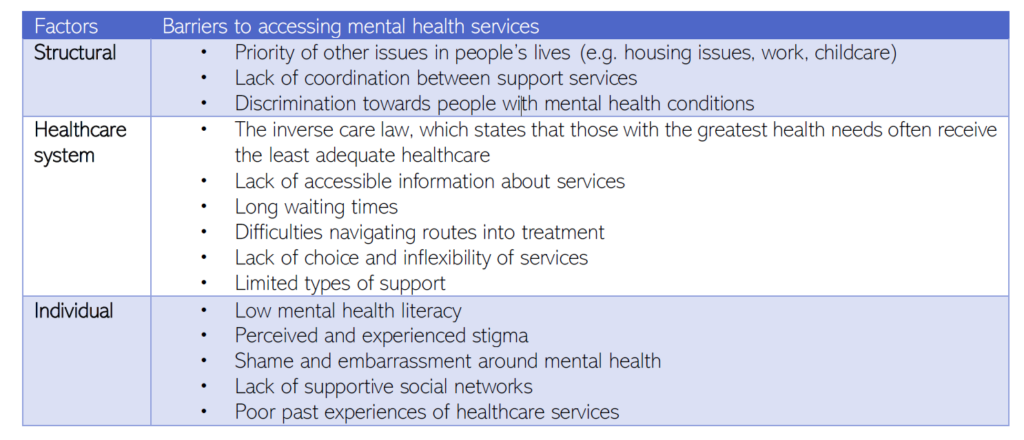
Common barriers to accessing mental health services
The groups below face common barriers to accessing mental health services. These barriers can be understood to act at 3 levels:
a) Structural factors: wider systemic factors.
b) Healthcare factors: features of healthcare staff and systems.
c) Individual factors: characteristics of individual people.
One the most significant barriers to accessing mental healthcare is stigma and discrimination.
- Internalised stigma occurs when people accept negative societal stereotypes and incorporate them into their own sense of self. This is associated with:
- Poorer quality of life (Livingston & Boyd, 2010).
- More severe psychiatric symptoms (Livingston & Boyd, 2010).
- Worse adherence to (Livingston & Boyd, 2010), and outcomes from (Thornicroft et al., 2022), mental health treatment.
- Stigma and discrimination around mental health conditions will be covered in more depth in future chapters.
Getting It Right First Time (GIRFT) states that trusts need to engage with patients and carers to identify and reduce avoidable barriers to patient access to mental health services, as well as ensuring that they have fast-track access to community mental health teams and other recognised best practices for referral and patient pathway routes.
- Trusts to provide access options such as email, text and video consultations, and other digital solutions for service users for whom telephone access is a barrier.
- Trusts to provide clear information on referral and access routes on the trust public website for each service.
- Trusts to work with local communities to ensure that potential barriers to access for any part of the community are identified and addressed to reduce inequity of service.
- Ensure that the national standards on accessible information are met.
A summary of interventions for reducing health inequalities in general practice found that general practice needs to be informed by five key principles, these can be applied widely when thinking about reducing inequalities in health services. The key principles were:
- involving coordinated services across the system (ie, connected),
- accounting for differences within patient groups (ie, intersectional),
- making allowances for different patient needs and preferences (ie, flexible),
- integrating patient worldviews and cultural references (ie, inclusive),
- engaging communities with service design and delivery (ie, community-centred)
Additional resources
- The local data pack gives an overview of key data and trends
- How to embed action on health inequalities into integrated care systems
- Health matters: reducing health inequalities in mental illness
- NIHR pages on how sociodemographic factors such as ethnicity, gender and sexuality and inequality are important in public mental health
- The Mental Health Foundation’s report Fundamental Facts About Mental Health
- Public mental health: Evidence, practice and commissioning gives of overview of inequalities
- Progress in improving mental health services in England
- Cambridgeshire Insight provides further information on local population groups
- Data on inequalities in the use of the Mental Health Act
- Inequalities in health care for people with depression and/or anxiety
- Building equitable primary care: A toolkit for practitioners and decision makers
- A national framework for NHS – Action on inclusion health
- NICE and health inequalities
- The Royal College of Psychiatrists – Health inequalities Briefing Pack and practical steps to reduce inequalities in mental health services and training in health inequalities
- OECD report on Understanding and Addressing Inequalities in Mental Health
- Mental Health 360 | Inequalities | The King’s Fund
References
Full list of references is included at the end of this chapter.