This mental health needs assessment aims to build the picture of mental health need across Cambridgeshire and Peterborough. If you are looking for information about looking after your own mental health, or that of someone you know, please go to Keep Your Head, which brings together reliable information on mental health and wellbeing for people in Cambridgeshire and Peterborough.
Please follow the links below to access each chapter of the mental health needs assessment. Each chapter is being added online as it is completed, and is constantly updated:
The overarching local strategy relating to health and wellbeing is the Health and Wellbeing and Integrated Care Strategy (2022-2030). This strategy was developed by the Joint Health and Wellbeing Board of Cambridgeshire County Council and Peterborough City Council, and aims to improve the health and wellbeing of the local population. It has three main goals: increasing the number of years people spend in good health; reducing inequalities in preventable deaths before age 75; and achieving better outcomes for our children.
Key definitions
- Mental health ‘exists on a continuum that can include periods of well-being and periods of distress, most of which will never evolve into a diagnosable disorder’ (1). Mental health conditions are symptoms that meet the criteria for diagnosis of a specific condition, although not everyone who experiences this will have received a diagnosis.
- Mental wellbeing is a subjective measure of how people feel about their lives. It can be defined using a range of measures, spanning people’s day-to-day satisfaction and happiness, to how they feel about their future.
- Mental health and wellbeing can be described as a continuum, where people can move between different levels of illness and wellbeing, depending on a range of factors.
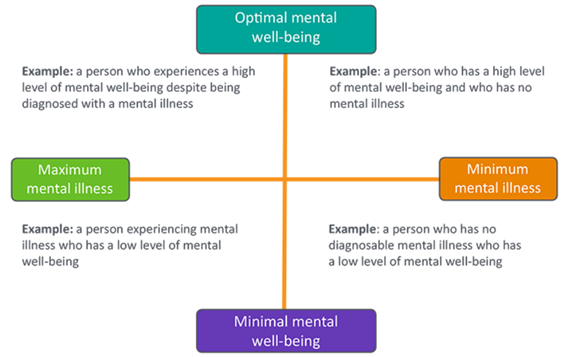
Figure 2: The relationship between mental health and wellbeing. Image source: Nottingham Mental Health Needs Assessment
Need, demand and supply are also important aspects of this mental health needs assessment. We have based our definitions of these terms on the work of Rice et al. (2021), who stated that:
- Need is the capacity to benefit from healthcare.
- Demand for healthcare is the level of healthcare use at which the perceived health benefits equal the cost of accessing care.
- Supply of healthcare is the services and treatments (both curative and preventative) provided by the health care system.
Parity of esteem between mental and physical health
- There are currently inequalities between physical and mental healthcare in the UK. Many sources describe these inequalities as falling under three themes (3):
- the preventable premature deaths of people with severe mental illnesses (the mortality gap)
- low rates of access to treatment for people with mental health conditions (the treatment gap)
- lower funding for mental health services relative to the level of need (the funding gap)
- Parity of esteem means that ‘mental health is viewed equally to physical health’. In 2024, this was defined for the NHS as ‘parity of timely access, evidence-based and therapeutic care, and patient experience for people with mental health needs’ (4).
- Some groups have criticised the term parity of esteem, arguing that this phrase can be unhelpfully vague, in that it does not set out a clear plan of action to address inequalities, or allow for mental health to be more important than physical health. Others state that issues of inequality between physical and mental health ‘can be better described as using concepts such as ‘discrimination’ and ‘social justice’ ’ (5).
Parity of esteem in policy
- Parity of esteem was first proposed in the England in the 2011 strategy ‘No Health Without Mental Health’ and was included in the Health and Social Care Act in 2012.
- Since then, NHS mandates have included objectives towards achieving parity, including setting a commitment to achieving parity by 2020, in the 2014 Five Year Forward View (6).
- The Department of Health and Social Care only provided a definition of what parity of esteem for mental health means for the NHS in 2024 (4).
How was the needs assessment written?
It is based on national research and data, local data the insights of local stakeholders and those with lived experience of mental health conditions. Following the structure recommended by Public Health England, it covers:
- Social and environmental factors important to public mental health,
- Population groups at higher risk of mental health conditions,
- Local mental health needs across the life-course.
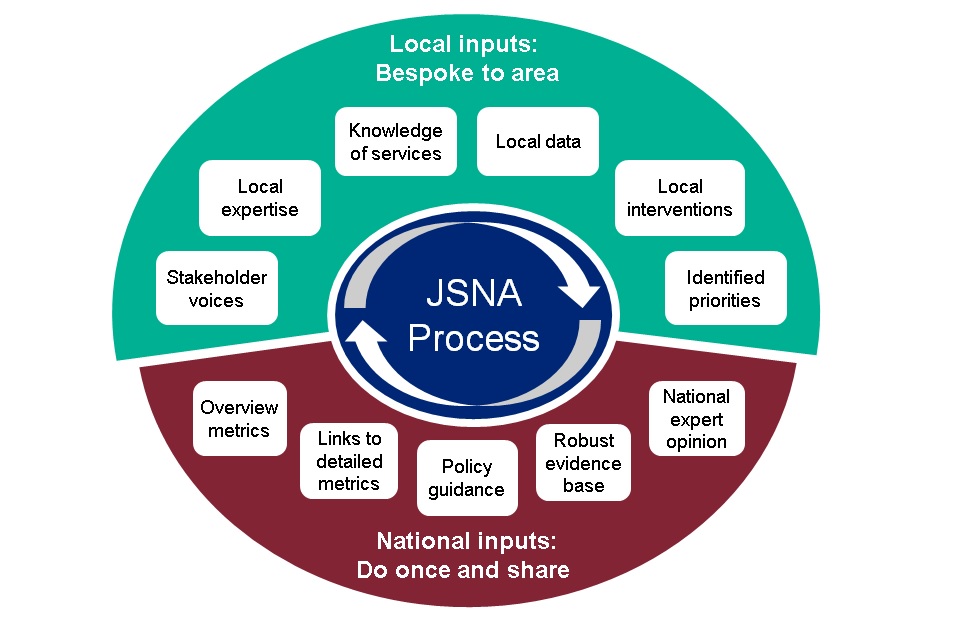
Figure 1: Collaboration model for JSNA development. Source: Public Health England
Each chapter involved use of an expert advisory group of local professionals, in order to shape the direction of this subsection, and to ensure that the needs assessment builds on previous work and knowledge. If you have questions about the data included in this needs assessment, please get in touch at phi-team@cambridgeshire.gov.uk
- Chapter One: There was no expert advisory group for this chapter
- Chapter Two: The substance use section of this chapter was developed with the help of an expert advisory group. This group included representatives from Local Authority, CPFT, Change Grow Live, Addenbrookes hospital, and the SUN Network. As a result of these conversations, and the findings of the 2023 Drug and Alcohol Needs Assessment, the focus for this section is on better understanding of the barriers people with co-occurring conditions may face when accessing mental health support.
- Chapter Three: The expert advisory group for perinatal mental health included professionals from children’s public health, maternity services, NHS Talking Therapies and the specialist perinatal mental health team.
- Chapter Four: The expert advisory group included professionals from child and adolescent mental health services, commissioning and the voluntary and community sector.
- Chapter Five: The expert advisory group included people with lived experiences of mental health services, healthcare professionals from CPFT, professionals from the voluntary and community sector and public health.
- Chapter Six: The expert advisory group included people with lived experience, healthcare professionals from CPFT, professionals from the voluntary and community sector and public health.
- Chapter Seven: The expert advisory group included people with lived experience, professionals from CPFT, professionals from the voluntary and community sector and public health. Particular thanks to Margaret Reed Roberts, who provided helpful comments on a draft copy of this report.
References
- UNICEF. On My Mind: Promoting, protecting and caring for children’s mental health [Internet]. 2021 [cited 2023 Jun 6]. Available from: https://www.unicef.org/reports/state-worlds-children-2021
- Campion J. Public mental health: Evidence, practice and commissioning. Royal Society for Public Health. 2019;(May).
- Mitchell AJ, Hardy S, Shiers D. Parity of esteem: Addressing the inequalities between mental and physical healthcare. BJPsych Adv. 2017;23(3).
- Wormald C. Correspondence from Sir Chris Wormald, Permanent Secretary, Department for Health and Social Care, re Sixty-fifth report of Session 2022-23, Progress in improving mental health services, dated 5 February 2024 [Internet]. DHSC; 2024 [cited 2024 Aug 28]. Available from: https://committees.parliament.uk/publications/43339/documents/215812/default/
- POST. Parity of Esteem for Mental Health [Internet]. 2015 [cited 2024 Aug 28]. Available from: https://www.transformationpartners.nhs.uk/wp-content/uploads/2018/04/Parity-of-Esteem-for-Mental-Health.pdf
- Baker C, Gheera M. Mental health: Achieving ‘parity of esteem’ [Internet]. 2020 [cited 2024 Aug 28]. Available from: https://commonslibrary.parliament.uk/mental-health-achieving-parity-of-esteem/