Mental Health JSNA
The Cambridgeshire and Peterborough Mental Health Needs Assessment was carried out between 2022 to 2024. This piece of work has been summarised in a Joint Strategic Needs Assessment (JSNA), with 15 key recommendations for the mental health system:
The full JSNA can also be viewed as a pdf.
How was this JSNA written?
This JSNA summarises the key findings and recommendations from the Cambridgeshire and Peterborough Mental Health Needs Assessment. These recommendations were prioritised in collaboration with system partners and were selected on the basis of their system-level impact on the Cambridgeshire and Peterborough mental health system.
Who was involved in the mental health needs assessment?
The Mental Health Needs Assessment was led by Kathryn Faulkner (Public Health Consultant at Cambridgeshire and Peterborough NHS Foundation Trust) and Kathy Hartley (Public Health Consultant at Peterborough City Council). It was produced by Eleanor Tovey (Public Health Manager), Saranya Palaniswamy (Public Health Advanced Analyst), Jamie Sheffield (Public Health Intelligence Analyst) and Agnes Toth (Lived Experience Co-ordinator). The chapter on suicide and self-harm was written by Tess Zermanos (Public Health Registrar) and led by Joe Davies (Suicide Prevention Manager) and Eleanor Tovey.
This report was guided by an advisory group of key stakeholders from the NHS, local authority, voluntary and community sector, as well as people with lived experience. These groups supported the prioritisation of recommendations in this JSNA.
How does this work overlap with other needs assessments and strategies?
There have been multiple local and national strategies in recent years calling for action on mental health. The findings of the Mental Health Needs Assessment reinforce the need to act on these recommendations, as detailed in the appendix of this report. In particular, the Mental Health Needs Assessment reinforces the four priorities of the Cambridgeshire and Peterborough Joint Health and Wellbeing Strategy (2022 – 2030):
- Our children are ready to enter and exit education prepared for the next phase of their lives
- Create an environment for people to be as healthy as can be
- Reducing poverty through better employment, skills and housing
- Promoting early intervention and prevention measures to improve mental health and wellbeing
It reaffirms that there remain substantial gaps in the provision of prevention and early intervention in mental health, as well as the importance of mental health communications, promoting positive relationships and action on the wider determinants of health.
Key principles and inequalities
Around 3 in 10 Cambridgeshire residents report that they struggled with their mental health in 2024 (1), which reflects the continuing impact of the COVID-19 pandemic and the rising cost of living (2,3). Furthermore, it has been estimated that mental ill-health costs the UK economy at least £118 billion each year, approximately 5% of the UK Gross Domestic Product (GDP) in 2019, predominantly due to the lost productivity of people with mental illness and costs incurred by unpaid carers (4). Comparatively, the NHS spent £16.8 billion on mental health services in 2023/23, including spend on learning disability, autism and dementia services (5).
Commit to parity of esteem
In Cambridgeshire and Peterborough, as well as nationally, the mental health system is under increasing pressure, with greater demand, longer waiting times and gaps in workforce and funding (6). Many people with mental health needs are waiting to receive support (7), or are not in contact with any NHS mental health services (7); and people with severe mental illness do not have access to the full range of evidence-based treatment. For example, there is no local community rehabilitation service to meet the needs of people with complex and enduring psychosis, and the treatment that is provided for severe mental illness is not equally accessible across the whole of Cambridgeshire and Peterborough. These unmet needs have a significant cost to individuals, families, communities and society (8). This reflects a lack of parity of esteem between physical and mental health: there are low rates of access to treatment for people with mental health conditions, compared to those for physical health; and lower funding for mental health services relative to the level of need (9).
Recommendation 1: The Integrated Care System should commit to parity of esteem between mental and physical health, to ensure that mental health is treated equally. This should include parity in terms of:
- prevention of mental health conditions
- access and provision of evidence-based treatment, particularly for severe mental illness, both in relation to need and across the geography of our local system
Integrate physical and mental healthcare
There are close links between poor mental health and physical health conditions. People with long-term physical health conditions are 2 to 3 times more likely to experience mental health problems than the general population (10). People with both physical and mental health conditions are more likely to experience poor outcomes, including greater rates of hospitalisation and less effective self-management (11); and 12 to 18% of NHS spending on long-term conditions is linked to poor mental health and wellbeing (12).
People with mental illness face physical health inequalities, including in terms of risk factors, early detection such as cancer screening (13) and health outcomes. In particular, people with severe mental health conditions face substantial physical health inequalities and die on average 15 to 20 years earlier than the general population (14). There is also a complex relationship between mental health and health behaviours, such as smoking, diet and exercise. For example, physical activity can act as a protective factor against a range of mental health conditions, including depression and anxiety, as well as reducing stress and improving self-esteem (15).
Recommendation 2: Strengthen efforts to integrate mental and physical healthcare, so that mental health is considered routinely in physical health interventions and vice versa for the physical health of people with mental illness. This should include a focus on people with severe and enduring mental illness.
Addressing poverty in services
Recent rises in child poverty, the cost of living and food insecurity, mean that an estimated 1 in 100 households in Cambridge and Peterborough live in destitution, a level of severe financial hardship which means that they struggle to meet their basic needs for shelter, food and heating (16,17). On top of this, there are over 47,000 children in Cambridgeshire and Peterborough living in poverty, ranging from 17% of children in East Cambridgeshire to over 30% in Peterborough and Fenland. This is a key driver of mental illness: research shows that socioeconomically disadvantaged children are 2 to 3 times more likely to develop mental health conditions (18). People with mental illnesses can be affected by a ‘spiral of adversity’, whereby their employment, income and relationships are negatively impacted by their mental health. This is often detrimental to their mental health condition and can trap them in poverty (19).
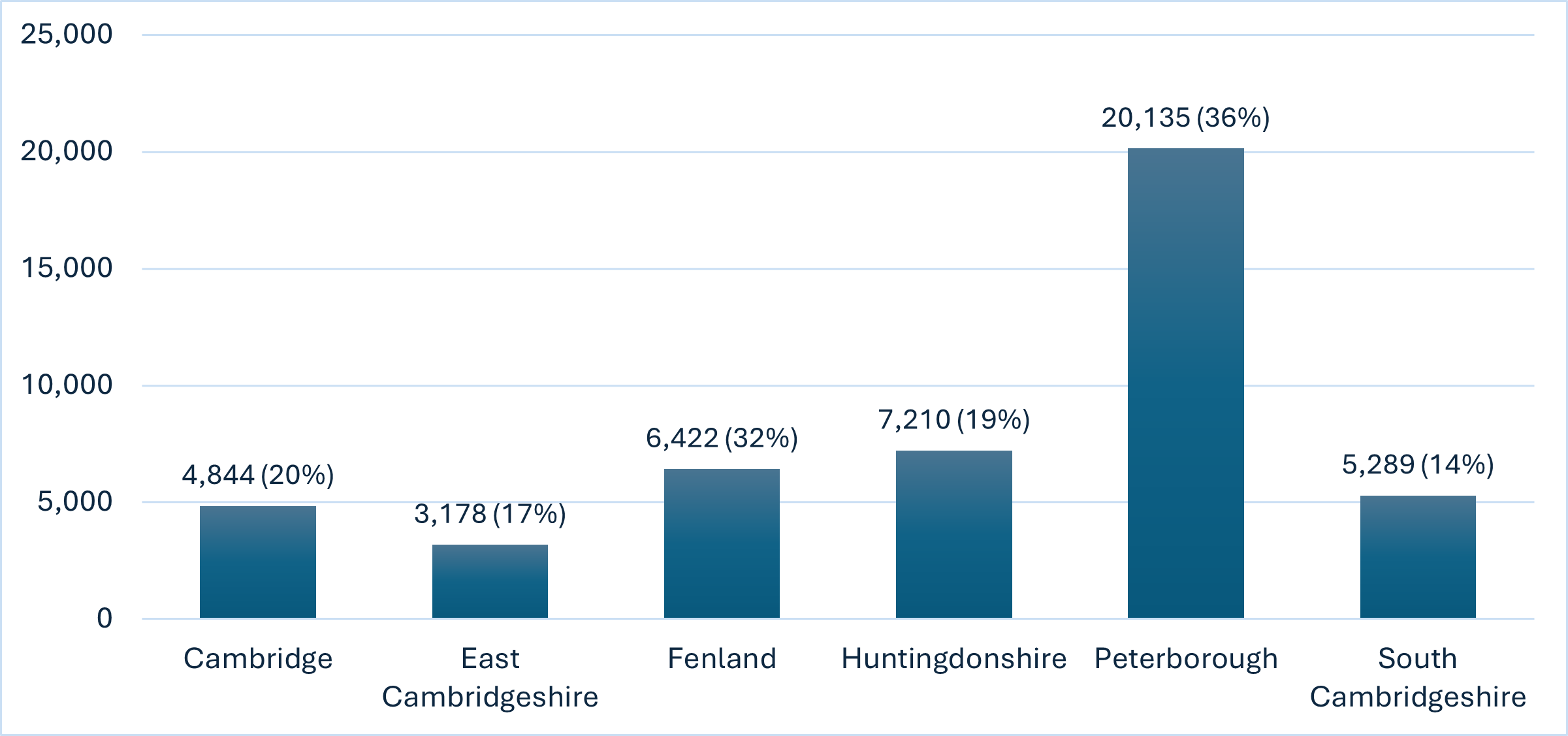
Figure 1: Number and percentage of children living in poverty, Cambridgeshire and Peterborough, 2022/23. Data source: End Child Poverty
The Marmot Review highlights that solely focusing on health behaviours is unlikely to reduce health inequalities (20). Instead, there should be a proportionate universalism approach, where action tackling health inequalities is universal but proportionate to the level of disadvantage. Services should respond to individuals’ health needs and social situation, including poverty; and provide increasing support as health inequalities increase (20).
There is ongoing work to understand and address poverty locally, including the Cambridgeshire County Council Poverty Strategy Commission and Peterborough Poverty Truth Commission. This should be built on within the Integrated Care System, to ensure that people living in poverty are not excluded from or further disadvantaged when accessing healthcare.
Recommendation 3: Ensure that people living in poverty are not disadvantaged when accessing mental healthcare and that services are able to maximise opportunities to address poverty.
Address wider determinants of health
The conditions in which we ‘are born, grow, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life’ are central to our mental health (21). Factors such as income, employment, deprivation, education and housing have been estimated to determine up to 55% of health outcomes (22). Our exposure to these wider determinants of mental health is ‘shaped by the distribution of money, power and resources at global, national and local levels, which are themselves influenced by policy choices’ (23). Action on these upstream factors is vital to the prevention of mental ill-health.
NHS organisations and local authorities can use their resources to influence the health of their local communities (24). Investment should be made in leadership and capacity so that organisations can maximise their impact on the wider determinants of health.
Recommendation 4: NHS organisations and local authorities are being increasingly recognised as ‘anchor institutions’, which can use their resources to influence the physical and mental health of their local communities. The system should work in partnership to develop system-wide anchor activities that maximise our social value impact.
Strengthen anti-racism
Health inequalities are ‘avoidable, unfair and systematic differences in health between different groups of people’ (25). In Cambridgeshire and Peterborough, there are stark inequalities in the wider determinants of health, risk factors, health care provision and clinical outcomes across socio-economic, disadvantaged and inclusion health groups (26). This is particularly true for mental health conditions, as some population groups are substantially more likely to experience mental ill-health. Much of these inequalities result from complex interactions of inequalities in wealth and power, including racism, misogyny, homophobia and other forms of injustice (27).
Local figures from Cambridgeshire and Peterborough show that there are substantial inequalities across all pathways of the mental health system, including by population group, age group and geographic area. For example, some services for people with treatment resistant depression, such as electroconvulsive therapy (ECT), are only available in some areas of the county. Local reports tell us that many autistic people and people with attention deficit hyperactivity disorder (ADHD) face barriers to accessing mental healthcare and difficulties navigating health services (28,29). Our survey of mental health professionals found that understanding of autism and ADHD and how they can interact with someone’s mental health, can be ‘hit and miss’.

Figure 2: Examples of inequalities in mental health in Cambridgeshire and Peterborough. Data sources: (30–33)
There have been decades of research highlighting ethnic inequalities in the prevalence of mental health conditions and across all aspects of the mental health system, including access to mental healthcare, discriminatory experiences of services and mental health outcomes (34). This is illustrated by the stark disparities in the rate of detentions under the Mental Health Act: people in England from ‘Any Other Black Background’ were 11 times more likely to be detained than people who are ‘White British’. Similar trends are seen in Cambridgeshire and Peterborough (35).
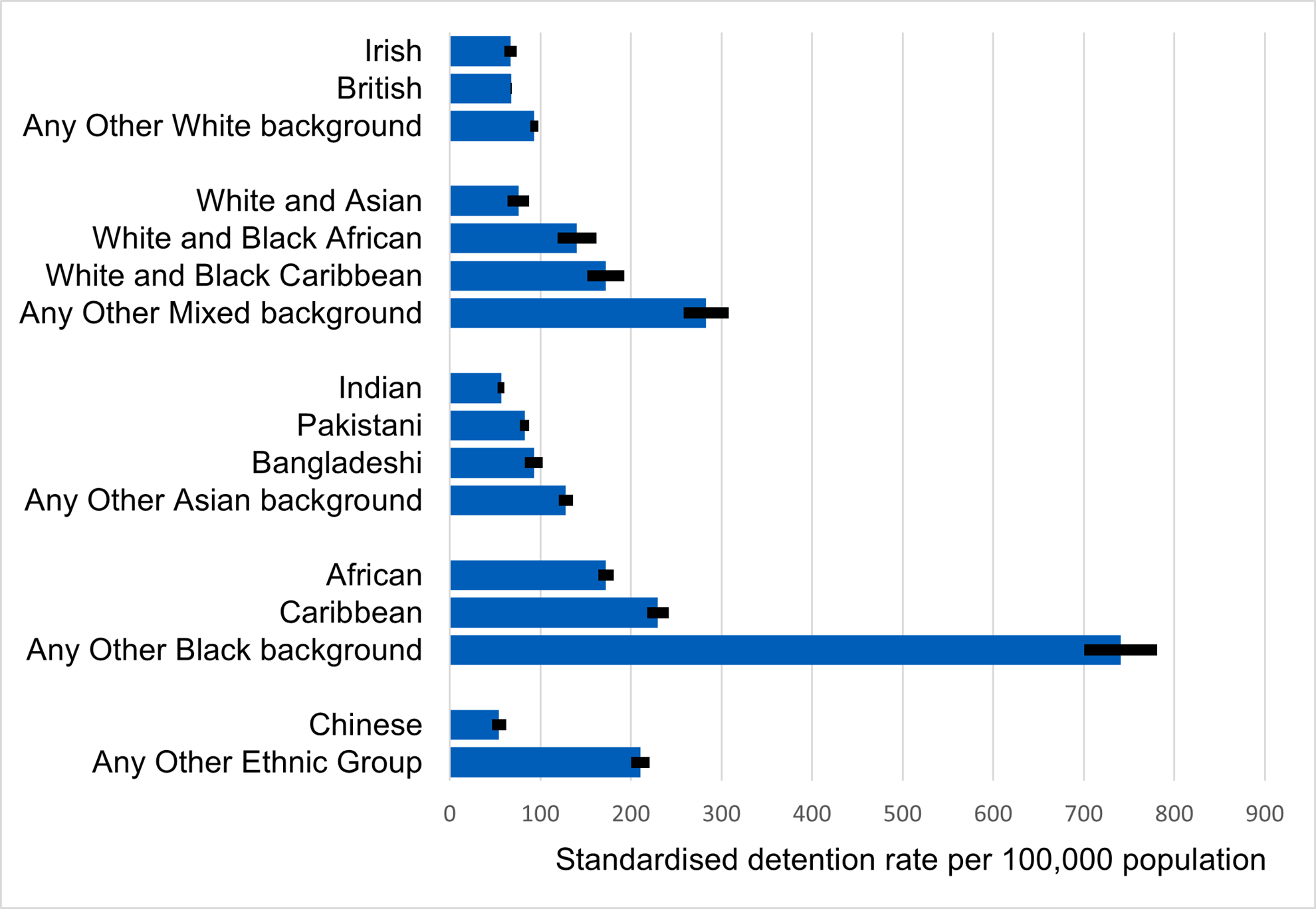
Figure 3: Rate of detentions under the Mental Health Act per 100,000 population by ethnic group, England, 2023-24. Image source: NHS Digital
These inequalities result from a complex interplay of social and economic inequalities, shaped by racism and discrimination (36). Understanding these inequalities and designing solutions to address them must stem from meaningful collaboration between healthcare services and local communities (37). Work has started in this area: Cambridgeshire County Council was the first upper tier local authority to commit to UNISON’s Anti-Racism Charter; and Cambridgeshire and Peterborough NHS Foundation Trust is actively working to implement NHS England’s anti-racism framework, the Patient and Carer Race Equality Framework (PCREF). This should be built on so anti-racism is embedded in all services, with coordinated work across the system to address root causes.
Recommendation 5: Recognise that tackling racism, including inter-personal, cultural, institutional and structural racism, should be a priority for improving mental health across the system. Strengthen leadership, action and accountability on anti-racism throughout all organisations in the Integrated Care System.
Meet the needs of people with co-occurring conditions
There is a close relationship between mental illness and substance use: around 60% of people in Cambridgeshire and Peterborough entering alcohol treatment have a recognised mental health need (38). Despite this, feedback collected by the local Service User Network (SUN) consistently highlights that people find it difficult to access joined up support across council-commissioned drug and alcohol treatment services and NHS-commissioned mental health services, including support for mental health needs in drug and alcohol services and support for substance use in mental health services. These findings were reiterated in the 2023 Drug and Alcohol Needs Assessment, which found that (38):
- Mental health support was the top issue raised by service users as missing from their support
- Over half of professionals working in local drug and alcohol service services felt that mental health provision for people with co-occurring conditions is ‘poor’, and fewer than 15% felt it was ‘good’ or ‘excellent’
- Every interview with professionals highlighted access to mental health support as a problem, including how a lack of access can lead to a ‘vicious circle’ of poor mental health and substance use

Figure 4: Professionals ratings of support for people who have co-occurring substance use and mental health issues. Data source: Drug and Alcohol Needs Assessment 2023
Whilst progress has been made in the provision of services, we need to build on success in this area to address unmet needs. For example, there is currently a gap in outreach, with existing teams mainly targeted to people experiencing homelessness. National guidance states that there are two key principles for services supporting people with co-occurring conditions: there should be a ‘no wrong door’ approach for people accessing support, and that meeting the needs of this group is ‘everyone’s job’ (39). Work towards these principles should be strengthened across the Integrated Care System.
Recommendation 6: Adopt the two key principles of ‘no wrong door’ and ‘everyone’s job’ across the system for people needing treatment for co-occurring substance use and mental health conditions. Strengthen partnership working across the system to ensure that we meet the needs of all people with co-occurring conditions, particularly those with severe mental illness.
System enablers
Build a learning health system
There is a lack of data insights in our mental health system. For example, we were only able to access limited data from general practices for this needs assessment, despite 30 – 40% of GP appointments having a mental health component (40,41). Data on inequalities and demographic factors such as ethnicity were often missing; and people’s experiences and outcomes from care were not integrated with other data or easy to access, as illustrated by physical health checks for people with severe mental illness. Whilst Cambridgeshire and Peterborough achieved the highest uptake rate of physical health checks for people with severe mental illness in the East of England in 2022/23, we are currently unable to monitor if this intervention improves people’s physical health, such as by supporting people to quit smoking, a leading cause of premature mortality for this group (42).
A learning health system is a systematic approach to data and improvement, by which commissioners and providers work with stakeholders to learn from routine care and improve as a result (43). We should develop learning health systems in mental health that integrate data from multiple sources, including the lived experience of people who use services.
Recommendation 7: Develop systems for all areas of the mental health system, which integrate data from a range of sources. Build the pool of expertise for mental health data analysis that is available across the Integrated Care System and more widely.
Recognise workforce as a priority
It is well-recognised that workforce is a major constraint to improving and expanding mental health services (6,44), due to issues with staff recruitment and retention, high turnover, and competition for staff from other healthcare providers (45). These workforce issues can make it difficult for staff and patients to build and maintain relationships (46), as well as having wider impacts across the whole mental health system, such as resilience of services. Clinical and operational staff are key for meeting all of the recommendations in this report.
This is illustrated by workforce issues leading to the closure of an adult mental health ward in Cambridgeshire in May 2022, with most beds only being reopened in November 2024. This ward closure contributed to a 20-fold increase in the number of patients placed in hospitals outside of their local area from April 2022 to 2023. The introduction of Integrated Care Systems provides an opportunity to develop an integrated workforce plan, that works across the health and care system to meet current and future population needs (47). This should include community services such as paediatrics, as well as staffing in the voluntary and community sector, and hospitals.
Recommendation 8: Develop a system-wide mental health workforce plan to address recruitment and retention issues. This should include establishment of new roles where appropriate, attention to cost of living issues and creative solutions in partnership with training bodies.
Invest in digital
Digital technologies and platforms, such as apps, online cognitive behaviour therapy and automated appointment reminders, have become a key part of mental health services. Effective implementation of these technologies is essential to meet system priorities, including helping people to manage their mental health, guiding care choices, tackling inequalities, reducing costs and freeing up staff time. However, digital approaches are not always used to their full potential (48) and can exacerbate inequalities faced by local people (49).
There is ongoing work in our system around digital technologies and platforms, including the community resource How Are You. Given our system’s need to prioritise workforce capacity in mental health, there should also be a focus on digital interventions that support capacity and enable staff to spend more time caring for patients.
Recommendation 9: Invest in, scale up and share digital operational tools across the Integrated Care System to release staff time. Embed evaluation in the roll out of digital technologies in mental health services.
Populations across the life course
Perinatal mental health (pregnancy and 0-2)
There were over 9,000 births in Cambridgeshire and Peterborough in 2023 (50). Pregnancy, birth and the first two years of a child’s life (known as the perinatal period) is a key period for families (51) and a critical time for the social, physical, emotional and language development of infants (52). Mental health conditions are some of the most common illnesses experienced over this time (53) and can have a significant impact on families, including the long-term mental health of parents (54) and children’s outcomes (55).

Figure 5: Impact of unidentified and untreated mental illness in the perinatal period
Up to 1 in 4 women and birthing people experience a mental health condition at the perinatal period (56), with 11 – 15% of new mothers in Cambridgeshire and Peterborough screening positive for depression within the first few months after birth. Wider determinants of health, including housing, poverty, racism, and gender-based violence, are the strongest upstream risk factors for poor mental health during the perinatal period (57). Past history of mental illness is also a strong risk factor, highlighting the importance of a life-course approach to mental health (58,59).
Most perinatal mental illness goes unrecognised, with 70% of individuals hiding or downplaying their illness (60), and only half of perinatal depression and anxiety cases being detected (61). Unlike other mental health contexts, almost the entire population of parents experiencing perinatal mental health difficulties have routine contact with health services, providing multiple opportunities for intervention. There is a particularly strong evidence base for investment in perinatal interventions to interrupt intergenerational transmission of inequalities: inadequate identification and treatment of perinatal depression, anxiety and psychosis costs society of £8.1 billion each year (53).
Align with perinatal priorities
In Cambridgeshire and Peterborough, there are a range of support services, ranging from those available to all parents and infants, such as the Healthy Child Programme, to services providing specialist perinatal mental health support. However, there are currently some gaps in provision.
The Cambridgeshire and Peterborough Perinatal and Infant Mental Health Network includes representatives from Public Health, Family Hubs, Cambridgeshire Community Services NHS Trust, Cambridgeshire and Peterborough NHS Foundation Trust, and voluntary and community sector organisations, as well as people with lived experience of perinatal mental health conditions. This group agreed on seven local priorities for perinatal mental health in 2022, which should refocus attention on this vital area of mental health and shape Integrated Care System work and planning:
- A robust antenatal education offer
- Dedicated support from a key contact during the perinatal period (up to age 2)
- Promoting strong parent-infant relationships
- Clear and supportive referral pathways
- Support for the whole family, including fathers, co-parents and partners
- Working with the wider system to tackle health inequalities and stigma
- Workforce training, development, and supervision
Recommendation 10: Deliver the 7 priorities for perinatal mental health for all.
Children and young people (aged 2 – 25)
There has been a rise in the number of children and young people in England who have diagnosable mental health conditions. In 2017, 1 in 9 children aged between 5 and 16 years had a probable mental health condition, which increased to 1 in 5 by 2023 (62). On top of this, more than half of young adults (aged 18 – 24) in Cambridgeshire often feel lonely (1). Experiencing poor mental health can have a substantial impact on young people’s lives, including on relationships, educational outcomes, and employment. Specialist mental health services for children and young people are not keeping up with this increasing demand, leading to growing waiting lists across England (63).
The Children and Young People’s JSNA highlights the growing complexity of children and young people’s needs. Some of these trends were emerging before the Covid-19 pandemic, but others were a direct impact of the pandemic response. The increasing levels of needs, alongside population growth for some local areas, have substantial implications for scale of demand, escalating costs, inequalities, and consequently, outcomes for children, young people, and their families.
Address any funding gap for children
Available evidence suggests that Cambridgeshire and Peterborough spending on children and young people’s mental health is lower than local Integrated Care Systems and is lower than the national average. While appreciating that benchmarking across different areas is complicated by different service configurations, categorisation of spend, and population health needs, Cambridgeshire and Peterborough spent £778 per child with an active referral to children and young people’s mental health services in 2022/23, the fifth lowest spend in England (64).

Figure 6: Integrated care board spend per head of total population on Children and Young People’s Mental Health (excluding learning disabilities and eating disorders), 2018/19 – 2022/23. Source: Mapping spend across children and young people’s mental health services Cambridgeshire and Peterborough
Recommendation 11: Undertake further analysis of children and young people’s mental health spend compared with other Integrated Care Systems in the East of England and other comparable areas nationally to ensure any gaps in investment are understood.
Meet the needs of young adults
Half of all mental health conditions become established before age 14, and 75% by age 24 (65). As shown in the graph below, the onset of severe and enduring mental health conditions, such as schizophrenia and eating disorders, often begins in late teenage years and early adulthood (66).
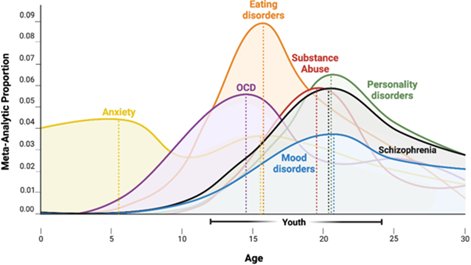
Figure 7: Age of onset of mental disorders. Image source: Towards a youth mental health paradigm: a perspective and roadmap
Currently YOUnited is the single point of referral for mental health and emotional wellbeing support in Cambridgeshire and Peterborough. Although Centre 33 accepts referrals up to age 25, most other YOUnited services limit referrals under 18s. As a result, young adults can fall through the gaps between children’s and adult services and can face a complicated route to accessing NHS mental health care. They report that they can face long waiting times for treatment and support, restrictive criteria that excludes them from accessing services, and difficulty accessing care that meets their intersecting needs (67).
Local data also shows that many young adults are currently presenting to our mental health service in crisis. Young adults aged 16 to 25 are the most frequent users of referrals to the First Response Service (FRS), and mental health is the leading reason why young adults frequently attend Accident and Emergency. This has a significant impact on individuals and their families, as well as a substantial cost to the system. The NHS Long Term Plan (2019) committed to extending service models to provide a ‘comprehensive offer’ of mental health support for 0- to 25-year-olds, that reaches across children and young people’s and adult mental health services (68). There is clear evidence and agreement locally for this 0-25 model for mental health support.
Recommendation 12: Develop a roadmap with system partners to extend services to meet the mental health needs of young people up to the age of 25, both for common mental health conditions and severe mental illness.
Working-age adults (aged 18 – 64)
Around two thirds of the population in Cambridgeshire and Peterborough are working-aged adults, aged between 16 and 64. It is predicted that there will be a 15.6% increase in the number of adults in this age group from 2021 – 2041. Mental illness is the largest cause of disability in this age group (69), and accounts for 11% of national social care spending for working-age adults (70).
1 in 6 adults experience depression and/or anxiety within any given week (71), which may have increased due to the wider impacts of the COVID-19 pandemic (3). Using this figure, an estimated 123,500 working-age adults in Cambridgeshire and Peterborough live with a common mental health condition. GP data shows 12% of adults are recorded as having depression and 0.8% a severe mental illness, with higher recorded rates of depression in Fenland (72).

Figure 8: Depression prevalence in adults as recorded by primary care, Cambridgeshire and Peterborough, 2016/17 – 2022/23. Data source: NHS Digital
Mental health services across England are under increasing pressure, including greater demand, the wider impacts of the COVID-19 pandemic (7) and challenges with staff recruitment and retention (6). Locally, there has been promising work to improve mental health services, including place-based approaches through North and South Place and the Integrated Neighbourhoods; the Community Mental Health Transformation, which addressed gaps in the mental health system and strengthened links between primary and secondary care services; and ongoing work to become a trauma-informed system.
However, feedback to the SUN Network highlights that some people experience long waiting times to access support (73). In particular, there is increasing demand for autism and ADHD assessments, which has led to a substantial increase in waiting times for these services.
At least 68,000 people across Cambridgeshire and Peterborough provide some level of unpaid care to someone with a long-term physical or mental health condition or problems related to old age (74), which is estimated to be worth around £1,500 million in Cambridgeshire, and £560 million in Peterborough (75). National surveys suggest that over a third of carers have a mental health problem and that 2 in 3 feel they need additional support to look after their own health and wellbeing (76,77).
Take action on crisis services
There are a range of support services for people experiencing mental health crisis in Cambridgeshire and Peterborough. Around 600 adults (aged 18+) a month attend Accident and Emergency due to a mental health emergency, an increasing proportion of whom spend over 6 hours in this department.
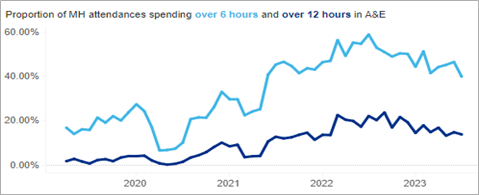
Figure 9: Proportion of adult (aged 18 – 64) mental health attendances spending 6+ and 12+ hours in Accident and Emergency, Cambridgeshire and Peterborough ICB, 2019 – 2023. Data source: Source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
A local review of review of the Mental Health Act ‘pathway’ in 2023 identified a range of system challenges, including gaps in crisis prevention, insufficient inpatient beds and delays in Mental Health Act assessments. Surveys of local professionals highlight gaps in the crisis system, particularly long waiting times to access support, a lack of early intervention and a range of services that are not well understood. This reflects national research, which has also found that crisis services can be over-subscribed and therefore inaccessible (78). Due to reports of local issues in crisis care, Cambridgeshire and Peterborough invested in a multiagency review of the mental health crisis pathway in Winter 2024.
Recommendation 13: Support implementation of the recommendations of the Crisis Pathway review and invest in co-designing the future approach.
Older adults (aged 65+)
Currently there are 160,000 older adults living in Cambridgeshire and Peterborough. By 2031, nearly 1 in 5 people will be aged 65+, with a significant rise in the number of people over 85 (79).

Figure 10: Actual and predicted number of older adults (aged 65+) in Cambridgeshire and Peterborough. Data source: 2023 JSNA
Healthy ageing strategy
As highlighted in the most recent Chief Medical Officer’s report, life aged 65+ is a period of great happiness for many people; whilst for others, it is a challenging period of discomfort, loss of independence and loneliness. The difference between these two outcomes is largely determined by physical and mental health: poor mental health is associated with considerable individual suffering, as well as social isolation, greater use of health and social care services and poorer physical health outcomes (80).
The 2023 JSNA stated that our ageing population should encourage the ‘whole system in Cambridgeshire and Peterborough to focus on prevention of ill health and disease’ (79). There should be a local healthy ageing strategy, which is a rights-based response to population ageing that promotes positive mental wellbeing (81). As there are common risk factors for multiple conditions (mental health, physical health, frailty and dementia) impacting older people, this will require a whole-system approach which addresses wider determinants of health (82). This should include dementia prevention, as an estimated 45% of dementia cases could be prevented by addressing 14 risk factors across the life course, many of which are associated with inequalities (83).
Recommendation 14: Work with local partners and communities to develop a healthy ageing strategy for Cambridgeshire and Peterborough.
Parity for older adults’ mental health
Around 14% of older adults have a mental health condition (84). Due to our ageing population, by 2040 the number of older adults with depression in Cambridgeshire is expected to rise by 26%, and 33% in Peterborough. Over the same period, the number of older adults with dementia will increase by 41% in Cambridgeshire and 47% in Peterborough (85).
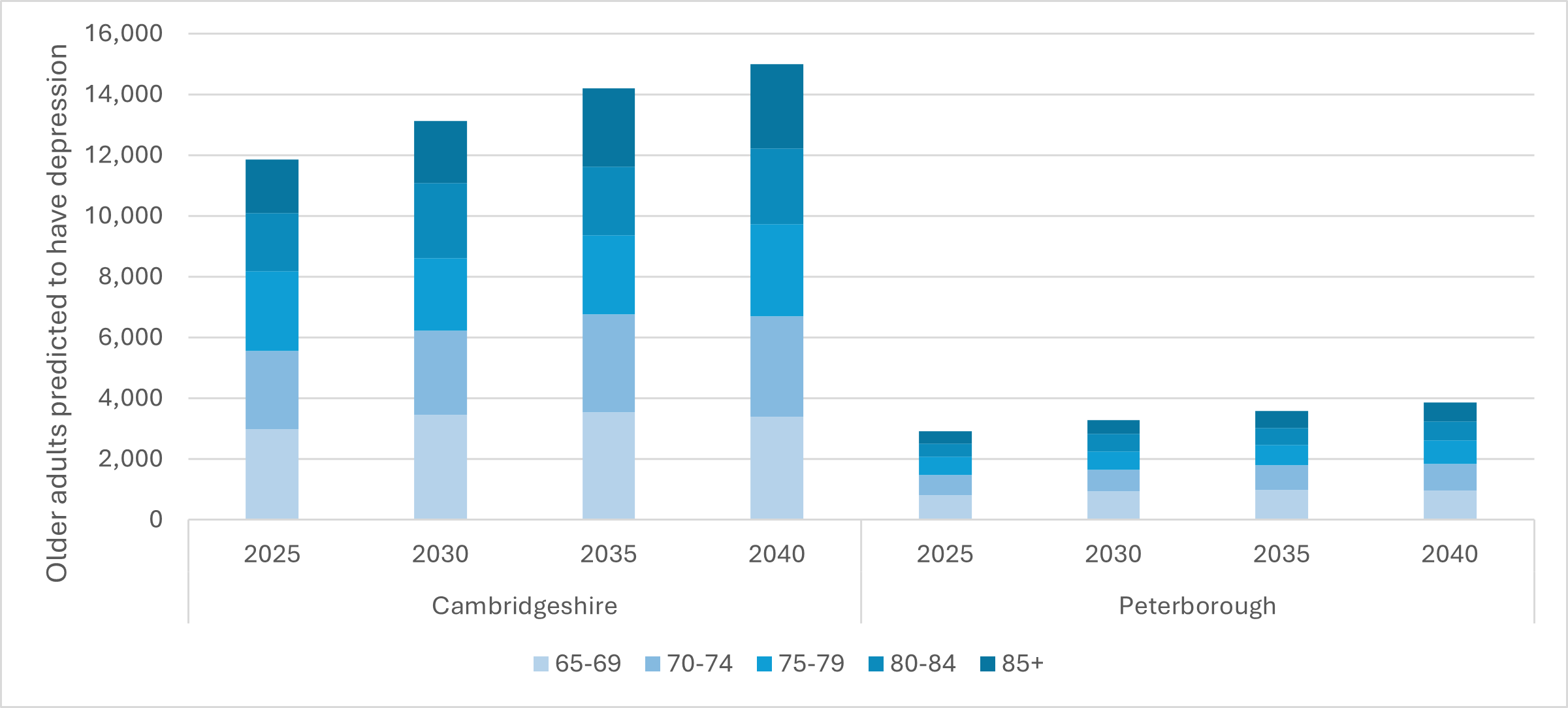
Figure 11: Older adults predicted to have depression, Cambridgeshire and Peterborough, 2020 – 2040. Data source: POPPI
Mental health is a key unmet need amongst older adults (86): compared to working-age adults, older people are more likely to experience mental health conditions but less likely to get timely access to care than working-age adults (87,88). This is reflected locally in feedback to the SUN Network, which reports that older adults face multiple barriers to accessing mental health support (89). Older adults have fed back that mental health support can be fragmented and prioritises dementia over conditions such as depression, anxiety, and personality disorder.
Older adults did not receive the same attention as working age adults in the Community Mental Health Transformation, as many of the services introduced do not support over 65s. Furthermore, the NHS recognises that healthcare professionals need to develop their knowledge to meet the needs of ageing populations with more complex needs (90). A lack of training for mental health professionals working with older adults can contribute to ageism in health and social care (91).
Recommendation 15: Ensure equity of access and treatments offered for older people with mental health conditions.
References
- Cambridgeshire County Council. Quality of life survey 2024 [Internet]. 2024 [cited 2024 Oct 2]. Available from: https://www.cambridgeshire.gov.uk/council/quality-of-life-survey-2024
- Office for National Statistics. Cost of living and depression in adults, Great Britain. 2022 [cited 2023 Aug 21]. Cost of living and depression in adults, Great Britain: 29 September to 23 October 2022. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/mentalhealth/articles/costoflivinganddepressioninadultsgreatbritain/29septemberto23october2022
- O’Shea N. Covid-19 and the nation’s mental health: May 2021 [Internet]. 2021 [cited 2023 Sep 7]. Available from: https://www.centreformentalhealth.org.uk/publications/covid-19-and-nations-mental-health-may-2021
- McDaid D, Park AL, Davidson G, John A, Knifton L, Morton A, et al. The economic case for investing in the prevention of mental health conditions in the UK. Mental Health Foundation. 2022;(February).
- NHS England. NHS mental health dashboard Q4 2022/23 [Internet]. 2023 [cited 2023 Nov 17]. Available from: https://www.england.nhs.uk/publication/nhs-mental-health-dashboard/
- Care Quality Commission. State of Care 2022/23 [Internet]. 2023 [cited 2023 Dec 11]. Available from: https://www.cqc.org.uk/publications/major-report/state-care/2022-2023
- Department of Health & Social Care. Progress in improving mental health services in England [Internet]. 2023 [cited 2023 Jun 13]. Available from: https://www.nao.org.uk/wp-content/uploads/2023/02/Progress-in-improving-mental-health-services-CS.pdf
- Jansen S, White R, Hogwood J, Jansen A, Gishoma D, Mukamana D, et al. The “treatment gap” in global mental health reconsidered: Sociotherapy for collective trauma in Rwanda. Eur J Psychotraumatol. 2015;6.
- Mitchell AJ, Hardy S, Shiers D. Parity of esteem: Addressing the inequalities between mental and physical healthcare. BJPsych Adv. 2017;23(3).
- Naylor C, Parsonage M, Mcdaid D, Knapp M, Fossey M, Galea A. Long-term conditions and mental health [Internet]. 2012 [cited 2022 Oct 11]. Available from: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/long-term-conditions-mental-health-cost-comorbidities-naylor-feb12.pdf
- Public Health England. Mental health and wellbeing: JSNA toolkit. 2019 [cited 2023 Aug 17]. Guidance: Working age adults. Available from: https://www.gov.uk/government/publications/better-mental-health-jsna-toolkit/6-working-age-adults
- Naylor C, Parsonage M, McDaid D, Knapp M, Fossey M, Galea A. Long-term conditions and mental health: the cost of co-morbidities. The King’s Fund and the Centre for Mental Health. Long-term conditions and mental health. 2012;
- National Institute for Health and Care Excellence. Health topics A to Z. 2023 [cited 2023 Nov 1]. Obsessive-compulsive disorder. Available from: https://cks.nice.org.uk/topics/obsessive-compulsive-disorder/
- Chesney E, Goodwin GM, Fazel S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry. 2014;13(2).
- Public Health England. 3. Mental health: population factors [Internet]. 2019 [cited 2022 Oct 14]. Available from: https://www.gov.uk/government/publications/better-mental-health-jsna-toolkit/3-understanding-people#fnref:43:2
- Earwaker R, Schmuecker K. Not heating, eating or meeting bills: managing a cost of living crisis on a low income [Internet]. 2022 [cited 2022 Sep 2]. Available from: https://www.jrf.org.uk/report/not-heating-eating-or-meeting-bills-managing-cost-living-crisis-low-income
- Joseph Rowntree Foundation. Destitution in the UK 2023 [Internet]. 2023 [cited 2024 Oct 29]. Available from: https://www.jrf.org.uk/deep-poverty-and-destitution/destitution-in-the-uk-2023
- Reiss F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Vol. 90, Social Science and Medicine. 2013.
- Public Health England. Mental health and wellbeing: JSNA toolkit. 2019 [cited 2022 Sep 5]. Mental health: environmental factors. Available from: https://www.gov.uk/government/publications/better-mental-health-jsna-toolkit/2-understanding-place
- Marmot M, Bell R. Fair society, healthy lives. Public Health. 2012;126(SUPPL.1).
- World Health Organisation. Social determinants of health [Internet]. 2022 [cited 2022 Sep 2]. Available from: https://www.who.int/health-topics/social-determinants-of-health
- Hood CM, Gennuso KP, Swain GR, Catlin BB. County Health Rankings: Relationships between Determinant Factors and Health Outcomes. Am J Prev Med. 2016;50(2).
- WHO. Taking action on the social determinants of health [Internet]. 2024 [cited 2024 Oct 8]. Available from: https://www.who.int/westernpacific/activities/taking-action-on-the-social-determinants-of-health
- NHS England. Anchors and social value [Internet]. 2024 [cited 2024 Oct 22]. Available from: https://www.england.nhs.uk/about/equality/equality-hub/national-healthcare-inequalities-improvement-programme/our-approach-to-reducing-healthcare-inequalities/anchors-and-social-value/
- Williams E, Buck D, Babalola G, Maguire D. What are health inequalities? [Internet]. 2022 [cited 2024 Oct 14]. Available from: https://www.kingsfund.org.uk/insight-and-analysis/long-reads/what-are-health-inequalities
- Ford J. Cambridgeshire and Peterborough Health Inequalities Strategy. 2020.
- Centre for Mental Health. Mental health for all? The final report of the Commission for Equality in Mental Health. Centre for Mental Health. 2020;(November).
- Cambridgeshire County Council, Peterborough City Council. Cambridgeshire and Peterborough All Age Autism Strategy 2021 – 2026 [Internet]. 2021 [cited 2023 Jan 20]. Available from: https://cambridgeshireinsight.org.uk/wp-content/uploads/2022/06/All-Age-Autism-Strategy-Full-Version-1.pdf
- Healthwatch Cambridgeshire, Healthwatch Peterborough. Autistic Voices: Local people’s health and care experiences [Internet]. 2021 [cited 2023 Jan 16]. Available from: https://www.healthwatchcambridgeshire.co.uk/sites/healthwatchcambridgeshire.co.uk/files/21%2004%20Autism%20Focus%20Group%20Final%20Report.pdf
- Lenhard J, Margetts M, Lund J, Varney A, Burgess G. Mapping healthcare barriers for people experiencing homelessness in Cambridge Report in collaboration with [Internet]. 2023 [cited 2024 Oct 8]. Available from: https://www.chirn.org/projects
- NHS Digital. Mental Health Act Statistics, Annual Figures, 2021-22 [Internet]. 2022 [cited 2023 Jan 12]. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-act-statistics-annual-figures/2021-22-annual-figures
- NHS Digital. NHS Talking Therapies data set reports [Internet]. 2024 [cited 2024 Oct 21]. Available from: https://digital.nhs.uk/data-and-information/data-collections-and-data-sets/data-sets/improving-access-to-psychological-therapies-data-set/improving-access-to-psychological-therapies-data-set-reports
- Healthwatch Cambridgeshire. Tackling Health Inequalities [Internet]. 2022 [cited 2024 Oct 21]. Available from: https://www.healthwatchcambridgeshire.co.uk/sites/healthwatchcambridgeshire.co.uk/files/202301%20Tackling%20Health%20Inequalities%20V2_0.pdf
- Kapadia D, Zhang J, Salway S, Nazroo J, Booth A, Villarroel-Williams N, et al. Ethnic Inequalities in Healthcare: A Rapid Evidence Review [Internet]. 2022 [cited 2022 Oct 26]. Available from: https://www.nhsrho.org/wp-content/uploads/2022/02/RHO-Rapid-Review-Final-Report_v.7.pdf
- NHS England. Mental Health Act Statistics, Annual Figures, 2023-24 [Internet]. 2024 [cited 2024 Nov 15]. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-act-statistics-annual-figures/2023-24-annual-figures
- Nazroo J. Race/ethnic inequalities in health: moving beyond confusion to focus on fundamental causes [Internet]. 2022 [cited 2022 Nov 29]. Available from: https://ifs.org.uk/inequality/wp-content/uploads/2022/11/Race-ethnic-inequalities-in-health-IFS-Deaton-Review-of-Inequality.pdf?utm_source=The%20King%27s%20Fund%20newsletters%20%28main%20account%29&utm_medium=email&utm_campaign=13599003_NEWSL_HWB_2022-11-21&dm_i=21A8,83H23,CEVEQA,X5EP5,1
- Turakhia P, Combs B. Using principles of co-production to improve patient care and enhance value. Vol. 19, AMA Journal of Ethics. 2017.
- Elvin D, Gallagher M, Jones D, Islan S, Webster R, Senker S, et al. Cambridgeshire and Peterborough Drug and Alcohol Needs Assessment 2023. 2023.
- Public Health England. Better care for people with co-occurring mental health and alcohol/drug use conditions: A guide for commissioners and service providers [Internet]. 2017 [cited 2022 Oct 24]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/625809/Co-occurring_mental_health_and_alcohol_drug_use_conditions.pdf
- Royal College of General Practitioners. Mental health in primary care [Internet]. 2017 [cited 2023 Aug 21]. Available from: https://www.rcgp.org.uk/representing-you/policy-areas/mental-health-in-primary-care
- Mind. GP mental health training survey Summary [Internet]. 2018 [cited 2023 Nov 16]. Available from: https://www.mind.org.uk/media-a/4414/gp-mh-2018-survey-summary.pdf
- Chesney E, Robson D, Patel R, Shetty H, Richardson S, Chang CK, et al. The impact of cigarette smoking on life expectancy in schizophrenia, schizoaffective disorder and bipolar affective disorder: An electronic case register cohort study. Schizophr Res. 2021;238.
- Hardie T, Horton T, Thornton-Lee N, Home J, Pereira P. Developing learning health systems in the UK: Priorities for action [Internet]. 2022 Sep [cited 2023 Nov 21]. Available from: https://www.health.org.uk/sites/default/files/upload/publications/2022/Learning%20health%20systems_RGB_WEB.pdf
- Health and Social Care Committee’s Expert Panel. Evaluation of the Government’s progress against its policy commitments in the area of mental health services in England [Internet]. 2021 [cited 2023 Oct 11]. Available from: https://publications.parliament.uk/pa/cm5802/cmselect/cmhealth/612/report.html
- House of Commons Committee of Public Accounts. Progress in improving NHS mental health services [Internet]. 2023 [cited 2023 Nov 17]. Available from: https://committees.parliament.uk/publications/40960/documents/199502/default/
- Care Quality Commission. The state of health care and adult social care in England 2021/22 [Internet]. 2021 [cited 2023 Sep 20]. Available from: https://www.cqc.org.uk/sites/default/files/2022-10/20221024_stateofcare2122_print.pdf
- NHS Employers. Integrated workforce thinking across systems: practical solutions to support integrated care systems (ICSs) [Internet]. 2022 [cited 2023 Nov 17]. Available from: https://www.nhsemployers.org/system/files/2023-09/integrated-workforce-thinking-across-systems-%281519%29.pdf
- Mental Health Network NHS Confederation. Maximising the potential of digital in mental health [Internet]. 2023 [cited 2023 Oct 20]. Available from: https://www.nhsconfed.org/system/files/2023-09/maximising-the-potential-of-digital-in-mental-health-%285996%29.pdf
- Healthwatch Cambridgeshire, Healthwatch Peterborough. Digital Inclusion report [Internet]. 2024 [cited 2024 Oct 22]. Available from: https://www.healthwatchcambridgeshire.co.uk/sites/healthwatchcambridgeshire.co.uk/files/202402%20Digital%20Inclusion%20report_0.pdf
- ONS. Births in England and Wales: summary tables [Internet]. 2024 [cited 2024 Oct 8]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/datasets/birthsummarytables
- Department of Health & Social Care. Best start for life: A Vision for the 1,001 Critical Days [Internet]. 2021 [cited 2023 Feb 21]. Available from: https://www.gov.uk/government/publications/the-best-start-for-life-a-vision-for-the-1001-critical-days
- Cumberlege J. Better Births – Improving outcomes of maternity services in England. The National Maternity Review. 2016;
- Bauer A, Parsonage M, Knapp M, Lemmi V, Adelaja B. The costs of perinatal mental health problems. LSE & Centre for Mental Health. 2014;(November).
- Vliegen N, Casalin S, Luyten P, Docx R, Lenaerts M, Tang E, et al. Hospitalization-based treatment for postpartum depressed mothers and their babies: Rationale, principles, and preliminary follow-up data. Psychiatry (New York). 2013;76(2).
- Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child. Vol. 384, The Lancet. 2014.
- Howard LM, Ryan EG, Trevillion K, Anderson F, Bick D, Bye A, et al. Accuracy of the Whooley questions and the Edinburgh Postnatal Depression Scale in identifying depression and other mental disorders in early pregnancy. British Journal of Psychiatry. 2018;212(1).
- Ormel J, Cuijpers P, Jorm AF, Schoevers R. Prevention of depression will only succeed when it is structurally embedded and targets big determinants. Vol. 18, World Psychiatry. 2019.
- Howard LM, Khalifeh H. Perinatal mental health: a review of progress and challenges. Vol. 19, World Psychiatry. 2020.
- Public Health England. Making the Case for Preconception Care: Planning and preparation for pregnancy to improve maternal and child health outcomes [Internet]. 2018 [cited 2023 Mar 2]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/729018/Making_the_case_for_preconception_care.pdf
- Maternal Mental Health Alliance. Perinatal mental health [Internet]. 2023 [cited 2023 Feb 2]. Available from: https://maternalmentalhealthalliance.org/about/perinatal-mental-health/
- Elliott I. Poverty and mental health: A review to inform the Joseph Rowntree Foundation’s Anti-Poverty Strategy. Mental Health Foundation. 2016;(August).
- NHS England. Mental Health of Children and Young People in England, 2023 – wave 4 follow up to the 2017 survey [Internet]. 2023 [cited 2024 Oct 22]. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2023-wave-4-follow-up
- Royal College of Psychiatrists. Record number of children and young people referred to mental health services as pandemic takes its toll [Internet]. 2021 [cited 2023 Jun 19]. Available from: https://www.rcpsych.ac.uk/news-and-features/latest-news/detail/2021/09/23/record-number-of-children-and-young-people-referred-to-mental-health-services-as-pandemic-takes-its-toll
- Children’s Commissioner. Children’s mental health services 2022-23 [Internet]. 2024 [cited 2024 Oct 8]. Available from: https://www.childrenscommissioner.gov.uk/resource/childrens-mental-health-services-2022-23/
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Vol. 62, Archives of General Psychiatry. 2005.
- Anderson JK, Newlove-Delgado T, Ford TJ. Annual Research Review: A systematic review of mental health services for emerging adults – moulding a precipice into a smooth passage. Vol. 63, Journal of Child Psychology and Psychiatry and Allied Disciplines. 2022.
- Taproot. Cambridgeshire and Peterborough Young People’s Mental Health Review. 2024.
- NHS. NHS Long Term Plan [Internet]. 2019 [cited 2023 Feb 8]. Available from: https://www.longtermplan.nhs.uk/
- Kirk-Wade E. House of Commons Library. 2022 [cited 2023 Jan 17]. UK disability statistics: Prevalence and life experiences. Available from: https://commonslibrary.parliament.uk/research-briefings/cbp-9602/
- The King’s Fund. Social care in a nutshell [Internet]. 2023 [cited 2023 Oct 25]. Available from: https://www.kingsfund.org.uk/projects/nhs-in-a-nutshell/social-care-nutshell
- NHS Digital. APMS. 2014. Adult Psychiatric Morbidity Survey: Survey of Mental Health and Wellbeing, England, 2014 – NHS Digital.
- NHS Digital. Quality and Outcomes Framework (QOF) [Internet]. 2023 [cited 2023 Nov 6]. Available from: https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/general-practice-data-hub/quality-outcomes-framework-qof
- Sidney L. Executive Directors Report – Quarter 1 – 2023/24 [Internet]. 2023 [cited 2023 Oct 31]. Available from: https://www.sunnetwork.org.uk/dev/wp-content/uploads/2023/07/Executive-Directors-report-Q1-2023-24.pdf
- Office for National Statistics. Unpaid care, England and Wales: Census 2021 [Internet]. 2023 [cited 2023 Jan 19]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/unpaidcareenglandandwales/census2021
- Petrillo M, Bennett M. Valuing Carers 2021 [Internet]. 2021 [cited 2023 Dec 18]. Available from: https://centreforcare.ac.uk/wp-content/uploads/2023/05/Valuing_Carers_WEB2.pdf
- Carers UK. State of Caring 2021 [Internet]. 2021 [cited 2022 Oct 19]. Available from: https://www.carersuk.org/images/Research/CUK_State_of_Caring_2021_report_web.pdf
- Sempik J, Becker S. Young Adult Carers at School: Experiences and Perceptions of Caring and Education Executive Summary. 2013.
- Healthwatch. Post pandemic: What are people telling us about mental health support? [Internet]. 2022 [cited 2023 Oct 31]. Available from: https://www.healthwatch.co.uk/blog/2022-07-07/post-pandemic-what-are-people-telling-us-about-mental-health-support
- PHI team. 2023 JSNA: Age structure and population change [Internet]. 2023 [cited 2024 Jan 23]. Available from: https://cambridgeshireinsight.org.uk/jsna-2023/demography/age-structure-and-population-change/
- Whitty C. Chief Medical Officer’s Annual Report 2023: Health in an Ageing Society [Internet]. 2023 [cited 2024 Jan 3]. Available from: https://assets.publishing.service.gov.uk/media/65562ff2d03a8d000d07faa6/chief-medical-officers-annual-report-2023-web-accessible.pdf
- World Health Organization. Decade of Healthy Ageing: baseline report. World Health Organization. 2020.
- The Association of Directors of Public Health. Policy Position: Healthy Ageing [Internet]. 2018 [cited 2024 Feb 20]. Available from: https://www.adph.org.uk/wp-content/uploads/2018/05/ADPH-Position-Statement-Healthy-Ageing.pdf
- Livingston G, Huntley J, Liu KY, Costafreda SG, Selbæk G, Alladi S, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Vol. 404, The Lancet. Elsevier B.V.; 2024. p. 572–628.
- GHDx. Institue for Health Metrics and Evaluation. 2023. Global Health Data Exchange.
- Institute of Public Care. Projecting Older People Population Information [Internet]. 2024 [cited 2024 Nov 12]. Available from: https://www.poppi.org.uk/
- Abdi S, Spann A, Borilovic J, De Witte L, Hawley M. Understanding the care and support needs of older people: A scoping review and categorisation using the WHO international classification of functioning, disability and health framework (ICF). BMC Geriatr. 2019;19(1).
- Davidson I. Mental Health – Adult Crisis and Acute Care GIRFT Programme National Specialty Report [Internet]. 2021 [cited 2023 Nov 17]. Available from: https://gettingitrightfirsttime.co.uk/wp-content/uploads/2021/09/Mental-Health-Sept21i.pdf
- Stickland N, Gentry T. Hidden in plain sight: The unmet mental health needs of older people [Internet]. 2016 [cited 2024 Jan 9]. Available from: https://www.ageuk.org.uk/globalassets/age-uk/documents/reports-and-publications/reports-and-briefings/health–wellbeing/rb_oct16_hidden_in_plain_sight_older_peoples_mental_health.pdf
- Sidney L. Executive Directors Report – Quarter 2 – 2023/24 [Internet]. 2023 [cited 2024 Jan 17]. Available from: https://www.sunnetwork.org.uk/dev/wp-content/uploads/2023/11/Executive-Directors-report-Q2-2023-24.pdf
- NHS England. NHS Long Term Workforce Plan [Internet]. 2023 [cited 2023 Nov 17]. Available from: https://www.england.nhs.uk/publication/nhs-long-term-workforce-plan/
- WHO. Global report on ageism [Internet]. Global Report on Psoriasis. 2021 [cited 2024 Feb 20]. 22–24 p. Available from: https://iris.who.int/bitstream/handle/10665/340208/9789240016866-eng.pdf?sequence=1