Crisis services
The mental health charity Mind has defined a mental health crisis as when some is in a ‘mental or emotional state where they need urgent help’ (Mind, 2011). Urgent, emergency and acute mental health care is provided by a range of teams and services (Public Health England, 2019), some of which may be used as part of planned care. This includes:
- Urgent metal health helplines: these services can be accessed by anyone and are open 24/7. They can assess people’s mental health and help people to access support.
- Crisis response and home treatment teams: these community-based services aim to assess and manage all patients in a mental health crisis and people also being considered for psychiatric hospital admission. They offer intensive home treatment rather than hospital admission, if this is safe and feasible.
- Mental health liaison services: situated in general hospitals, for example in the emergency department or inpatient wards, these services aim to provide psychiatric assessment and treatment to patients who may be experiencing mental health conditions whilst in hospital.
- Acute inpatient services: provide treatment when a person’s mental health condition cannot be managed in the community, and where the situation is so severe that specialist care in a safe and therapeutic space is required.
The NHS Long Term Plan set aims for significant expansion to crisis services, which should allow faster access for people experiencing mental health crisis (NHS, 2019).
Getting It Right First Time
The GIRFT vision is that people accessing services will:
- be treated as equals and as partners in their assessment, care and treatment.
- given copies of their assessments, so that they can check and correct them if necessary, and see that they have not only been listened to but heard correctly.
- get information on the current known outcomes and potential benefits and harms of any proposed intervention.
- not be repeatedly asked to give their history unless there is a clear and specific need to clarify something in the assessment or therapy.
- routinely be asked their opinion on aims and desired outcomes of accessing the service, and whether the interventions were beneficial to them, taking into account any harms from the intervention (i.e. was there a net positive benefit for them).
- Sometimes the treating team and person accessing the service may disagree on issues identified or desired aims and outcomes. Such disagreements should be routinely noted and where feasible agreed compromises reached.
In Cambridgeshire and Peterborough, nationally monitored indicators suggest there are particular pressures on inpatient services. There are likely to be a range of factors contributing to this, such as workforce pressures which led to the closure of the Mulberry Ward 3. Greater acuity of mental health need at the point of admission and delays to discharge may also contribute.
Overview of community crisis services
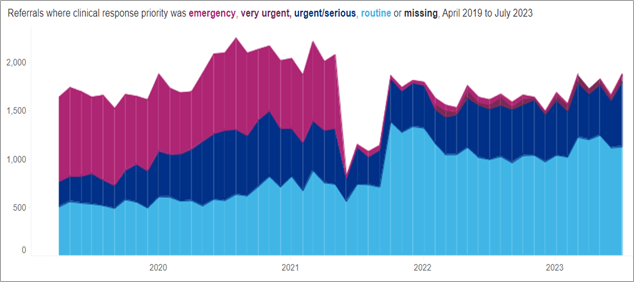
Note that there was a change in data systems in adult and specialist mental health services on 14th June 2021, hence some national dashboards show a substantial spike around these dates.
There has been a substantial decline in the number of referrals to community crisis services which are classified as ‘emergency’ since 2021. There were 215 ‘emergency’ referrals in the 12 month period ending July 2023, 59% lower than the previous 12 months (520).
Figure 32: Referrals to community crisis services, 18-64 years, Cambridgeshire and Peterborough ICS, April 2019 – July 2023. Data source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
Referrals are classified using the following criteria:
- Emergency: emergency situations in which there is imminent risk to life or serious harm to themselves or others and will require a “999” response, potentially within minutes. This would require a response from the police or an ambulance, but may also require rapid support or a joint response from a mental health crisis service.
- Very urgent: people who present a risk of harm to themselves or others; present acute suicidal ideation with clear plan and intent; have a rapidly worsening mental state; do not require immediate physical health medical intervention; are not threatening violence to others. These referrals require a very urgent face-to-face assessment with a specialist mental health crisis practitioner within 4 hours.
- Urgent: typical presentations in this category include high risk behaviour due to mental health symptoms; new or increasing psychiatric symptoms that require timely face-to-face intervention to prevent full relapse; significantly impaired ability for completing activities of daily living; vulnerability due to mental illness; expressing suicidal ideation but no plan or clear intent. These referrals require an urgent face-to-face assessment with a specialist mental health crisis practitioner within 24 hours.
- Routine/non-urgent: in the context of crisis care, this term covers all responses that do not require an urgent face-to-face intervention from a specialist NHS mental health crisis service.
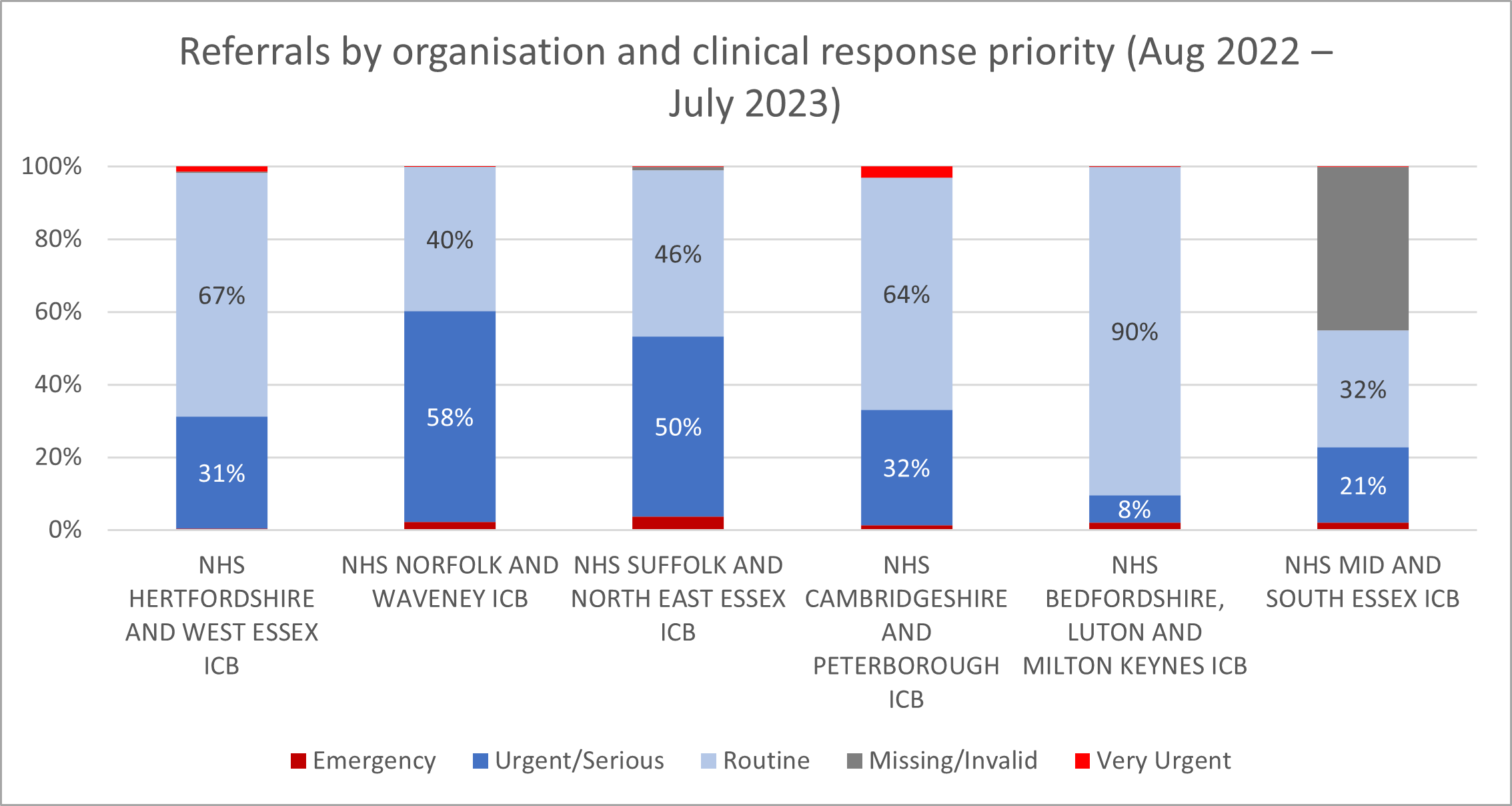
For the year ending July 2023, Cambridgeshire and Peterborough had 64% routine, 32% urgent or serious, 3% very urgent and 1% emergency referrals. There is substantial range in the types of referral across the East of England.
Figure 33: Referrals to community crisis services by clinical response priority, 18-64 years, East of England, August 2022 – July 2023. Data source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
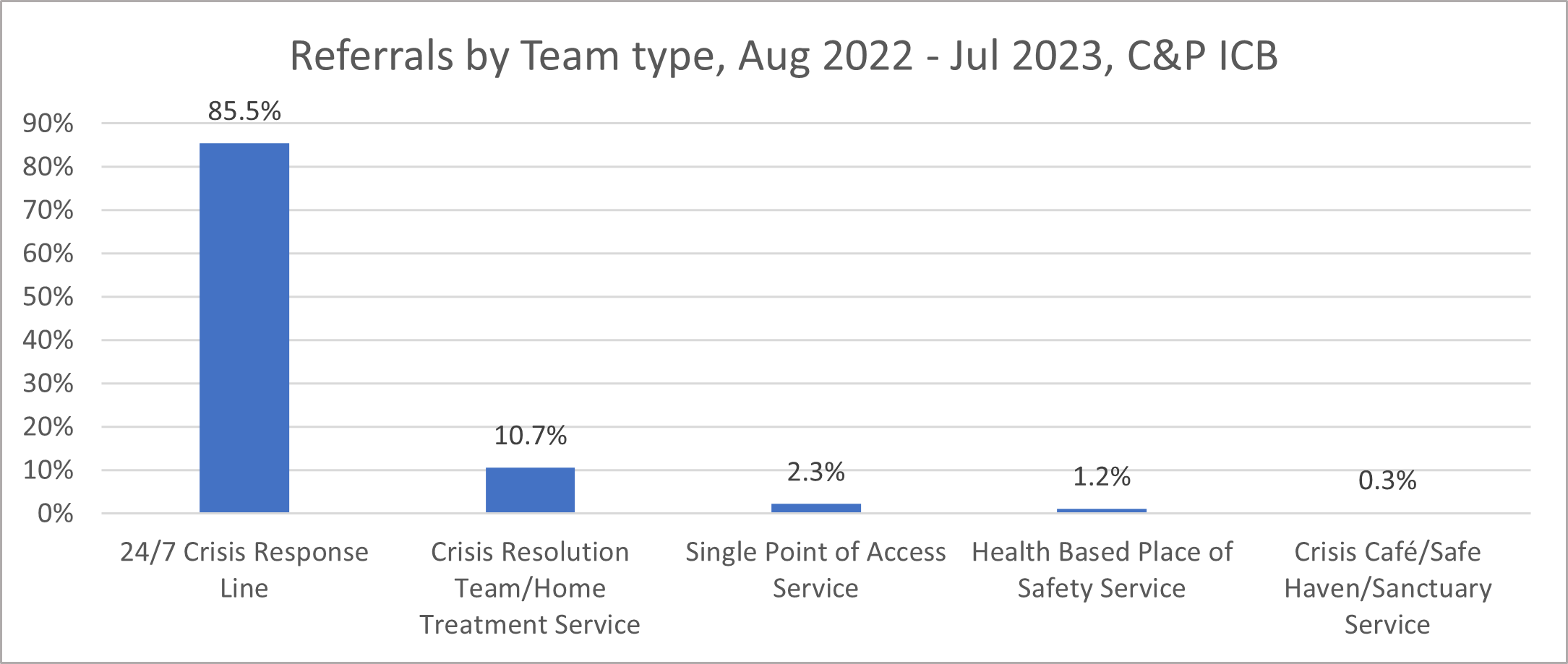
Local data shows that the First Response Service (FRS, a 24/7 crisis response line) is a well-established part of the crisis pathway in Cambridgeshire and Peterborough. From August 2022 to July 2023, FRS received 86% of referrals into community mental health crisis services.
Figure 34: Referrals to Community Crisis Services by team type, 18-64 years, Cambridgeshire and Peterborough ICS, August 2022 – July 2023. Data source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
Experience of crisis services
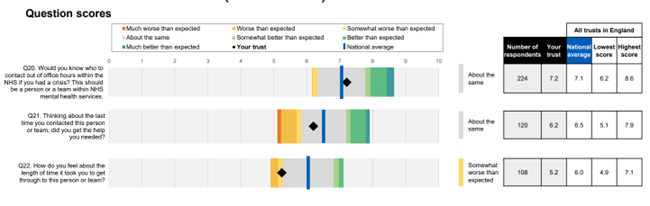
The NHS Community Mental Health Survey (2022) included three questions around crisis care:
- There was a significant decrease in the scores for each of these questions in Cambridgeshire and Peterborough from 2021 to 2022, showing that people had poorer experiences.
- People’s feelings on the ‘length of time it took to get through to the person or team providing support’ was scored 5.2 out of 10 and was highlighted as a key area for improvement. This score was somewhat lower than other areas in England.
Figure 35: Experiences of crisis services as reported in the NHS Community Mental Health Survey. Image source: NHS Community Mental Health Survey Benchmark Report 2022
There is limited research looking into access or experience of crisis services by autistic people and people with ADHD (Balazs and Kereszteny, 2017; Cassidy et al., 2018). One American study found that autistic adults were 2.6 times more likely to attend Accident and Emergency because of their mental health than non-autistic adults (Vohra, Madhavan and Sambamoorthi, 2016); however, a recent review did not identify any studies looking into autistic people’s access to or experience of mental health crisis lines (Cleary et al., 2022).
First response service
The First Response Service (FRS) provides support for people experiencing a mental health crisis and is available 24/7. Support offered can include telephone support, a face-to-face assessment and referrals to other CPFT services. A detailed analysis of FRS service use from August 2021 and March 2023 found that:
- There is annual variation in FRS rates of referrals, with between 1,600 to 1,900 people being referred each month.
- The greatest rates of referrals were from people in their late teens to early thirties.
- More women than men accessed this service.
- There were higher referral rates amongst ‘White’ ethnic groups than other ethnic groups.
- Referrals to FRS were higher in Cambridge and Peterborough compared to other districts. Referral rates were also higher in more deprived areas.
Full results of this analysis are summarised below.
How many people are referred to FRS?
The number of unique referrals accessing FRS each month ranged from over 1,900 in October 2021, to below 1,600 in April 2022. There was a trend towards lower number of referrals from August 2021 to December 2023, although there was a spike in March 2023.
Figure 36: Total number of referrals accessing FRS by month, August 2021 – March 2023. Data source: FRS analysis
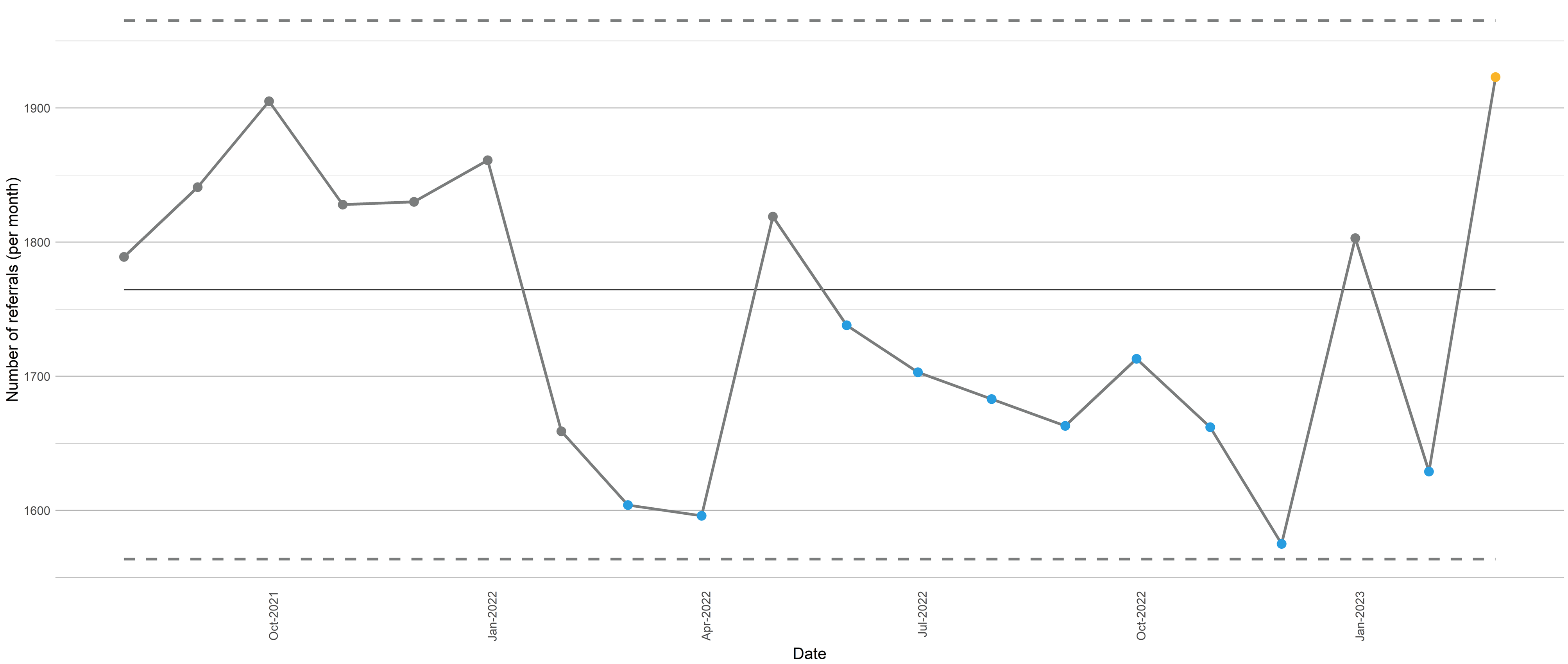
Note: this is a statistical processes control (SPC) chart. The horizontal black line represents the mean over the baseline period. The dotted lines on either side of the mean are the control limits, which represent the threshold between normal variation in the data and variation that is beyond the range that we would expect.
- The mean and control limits are calculated based on the first 12 points of time plotted.
- The yellow dots represent data points of concern, either due to the distance from the norm or because the performance has been worse for a substantial amount of time (7 measurements in a row); whilst blue dots represent data points where performance is considerably better than then norm, or performance has been better for a substantial amount of time (7 measurements in a row).
Who is referred to FRS?
- The greatest rates of referrals come from people in their late teens to early thirties.
- There are more referrals for women than men; and higher referral rates amongst ‘White’ ethnic groups than other ethnic groups.
- In terms of geographic variation, referrals are higher in Cambridge and Peterborough compared to other districts, and also higher in more deprived areas.
- Some general practices and primary care networks have above or below average referral rates to FRS, but the reasons behind this are unclear.
Where are referrals from?
The vast majority of referrals to FRS are self-referrals; followed by from GPs, internal referrals (where referrals are labelled as coming from 111, ‘First Response Service’ or ‘Internal Referral’) and relatives or carers. For these more common pathways, between 1% to 6% of referrals lead to a face-to-face contact.
What happens after people are referred to FRS?
The triage category refers to the time they need to be assessed by a member of the clinical team. Approximately 86% of referrals to FRS are for advice; after this most people are triaged within 24 hours.
Referrals for advice from ‘Asian or Asian British’ service users are lower than all other groups; whilst referrals for advice from service users from ‘white’ ethnic groups are higher. For other triage categories, referral numbers are too low to draw any conclusions about potential inequalities by ethnicity.
What is the profile of high service users?
There is a small number of people accessed this service multiple times from August 2021 to March 2023. This analysis looked at the 1112 people who were in the 90th to 98th percentile of referrals, individuals who had between 4 to 11 referrals between this period. This group is more likely to be female and from younger age groups, compared to all people who have used FRS. The rate of high service users is comparable across most ethnic groups; but some GPs have higher numbers of high service users.
There is a small number of people who have a very high level of service use. This analysis looked at the 278 people who were in the 99th to 100th percentile of referrals, individuals who had between 12 to 580 referrals between August 2021 and March 2023. Similar to the high service use group, this group of individuals was more likely to be female and most ethnic groups have similar rates to the total group of people using FRS. A few GPs have higher numbers of individuals with very high levels of service use. There was a relatively even distribution by ages.
Crisis response and home treatment teams
The crisis resolution and home treatment team (CRHTT) is a 24/7 service that provides intensive support to people experiencing mental health crisis. They offer intensive home treatment rather than hospital admission, if this is safe and feasible. They also work to facilitate early discharge from hospital where possible and appropriate (Public Health England, 2019).
Where are people referred from?
- Referrals to this service are made from other mental health services, including the First Response Service (FRS). Most referrals are from Accident and Emergency (through Liaison Psychiatry), the community mental health team (adult locality teams) and adult inpatient mental health services.
- Around 87% of referrals to CRHTT lead to a face-to-face contact, a rate that has remained relatively stable since June 2021.
- The rate of referrals resulting in a face-to-face contact is higher for referrals from inpatient adult mental health services and First Response Service (over 75%), and lower for referrals from Accident and Emergency (around 50%).
Figure 37: Percentage of unique referrals accessing CHRTT resulting in a face-to-face contact, June 2021 – August 2023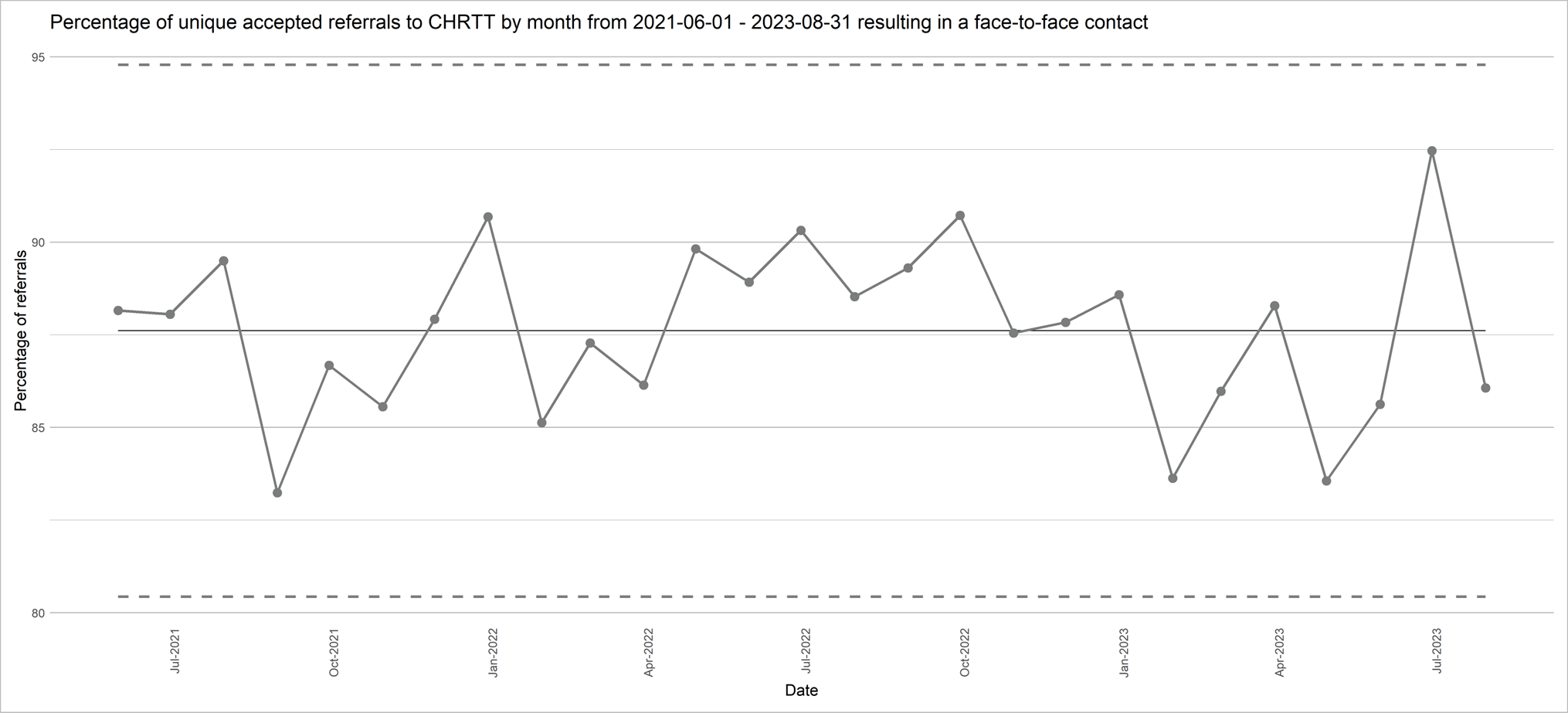
Who is referred to this service?
From June 2021 to August 2023:
- A similar rate of men and women were referred to CRHTT.
- People from the most deprived were more likely to be referred to this service, compared to those from less deprived areas.
- There was a particularly high rate of referrals to the CRHTT for people in their early twenties in Cambridgeshire and Peterborough. There was also a low rate of referrals for people over 65.
- A higher rate of people were referred to the CRHTT from Cambridge City and Peterborough, and lower from East Cambridgeshire, compared to other districts.
- People from ‘Black or Black British’ ethnic groups were substantially more likely to be referred to the CRHTT than people from other ethnic backgrounds.
Ambulance
Ambulances respond to people in serious medical emergencies, including those experiencing a mental health crisis and people who have self-harmed.
A mental health response car was introduced across Cambridgeshire and Peterborough in 2021. This service is for people who call 999 when experiencing a mental health crisis and is staffed by a paramedic and specialist mental health practitioner. This was introduced as a joint initiative between Cambridgeshire and Peterborough NHS Foundation Trust (CPFT) and East of England Ambulance Service (EEAST) (99).
Accident and Emergency
Accident & Emergency departments (A&E or Emergency Departments) support people facing serious or life-threatening medical emergencies, including those experiencing a mental health crisis and people who have self-harmed.
How many people attend Accident and Emergency for mental health reasons?
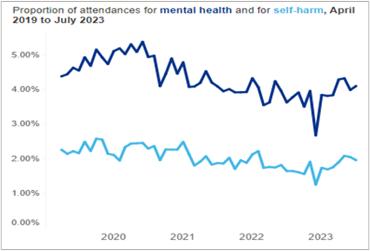
In Cambridgeshire and Peterborough ICS, the proportion of Accident and Emergency attendances for mental health and for self-harm have increased since December 2022.
Figure 38: Proportion of Accident and Emergency attendances for mental health and self-harm, Cambridgeshire and Peterborough ICS, April 2019 – July 2023. Image source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
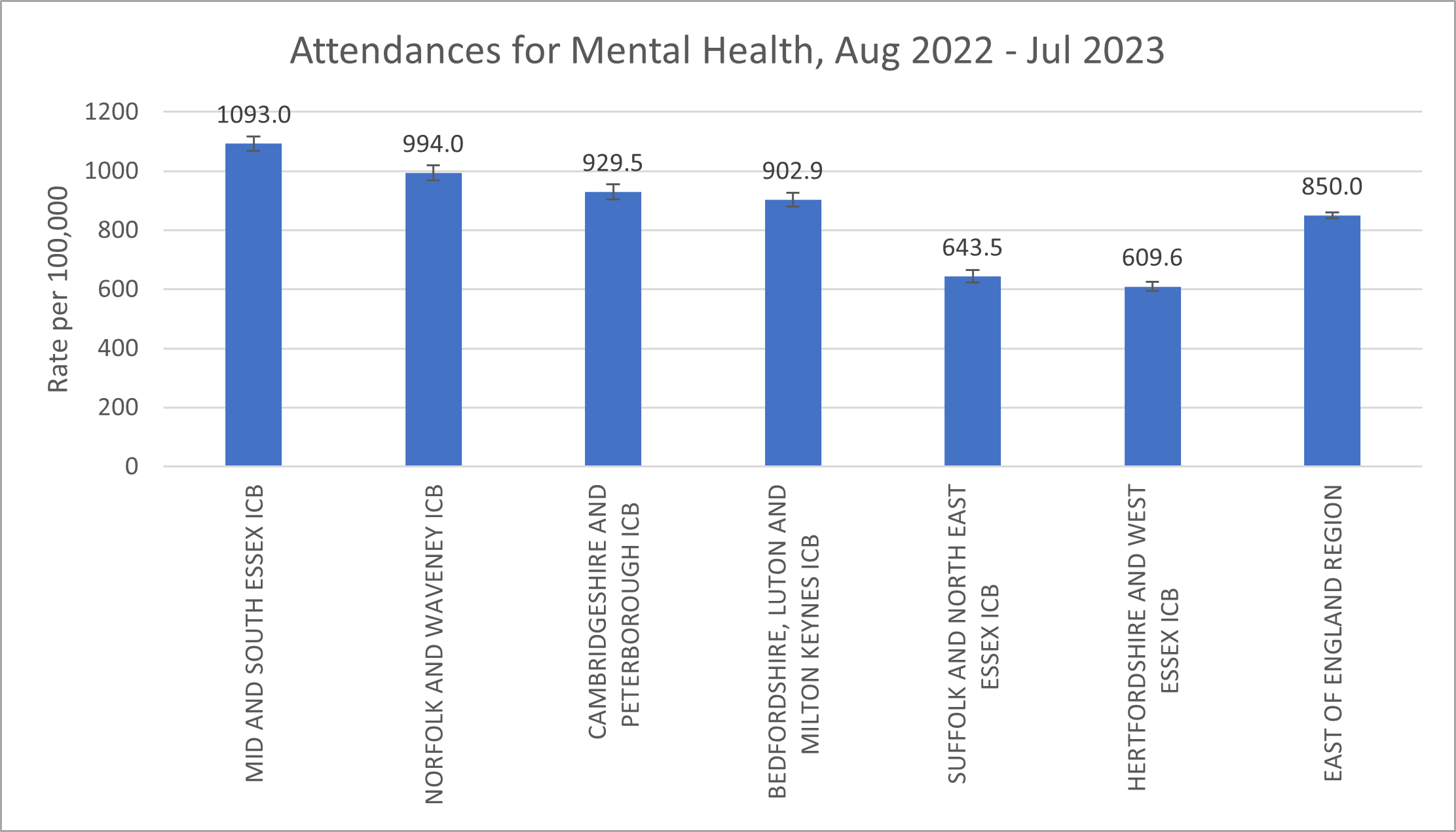
Rates of attendances to Accident and Emergency where the primary complaint was mental health-related (including self-harm) in Cambridgeshire and Peterborough are similar to other areas in the East of England.
Figure 39: Accident and Emergency attendances for mental health, Cambridgeshire and Peterborough ICS, August 2022 to July 2023. Source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
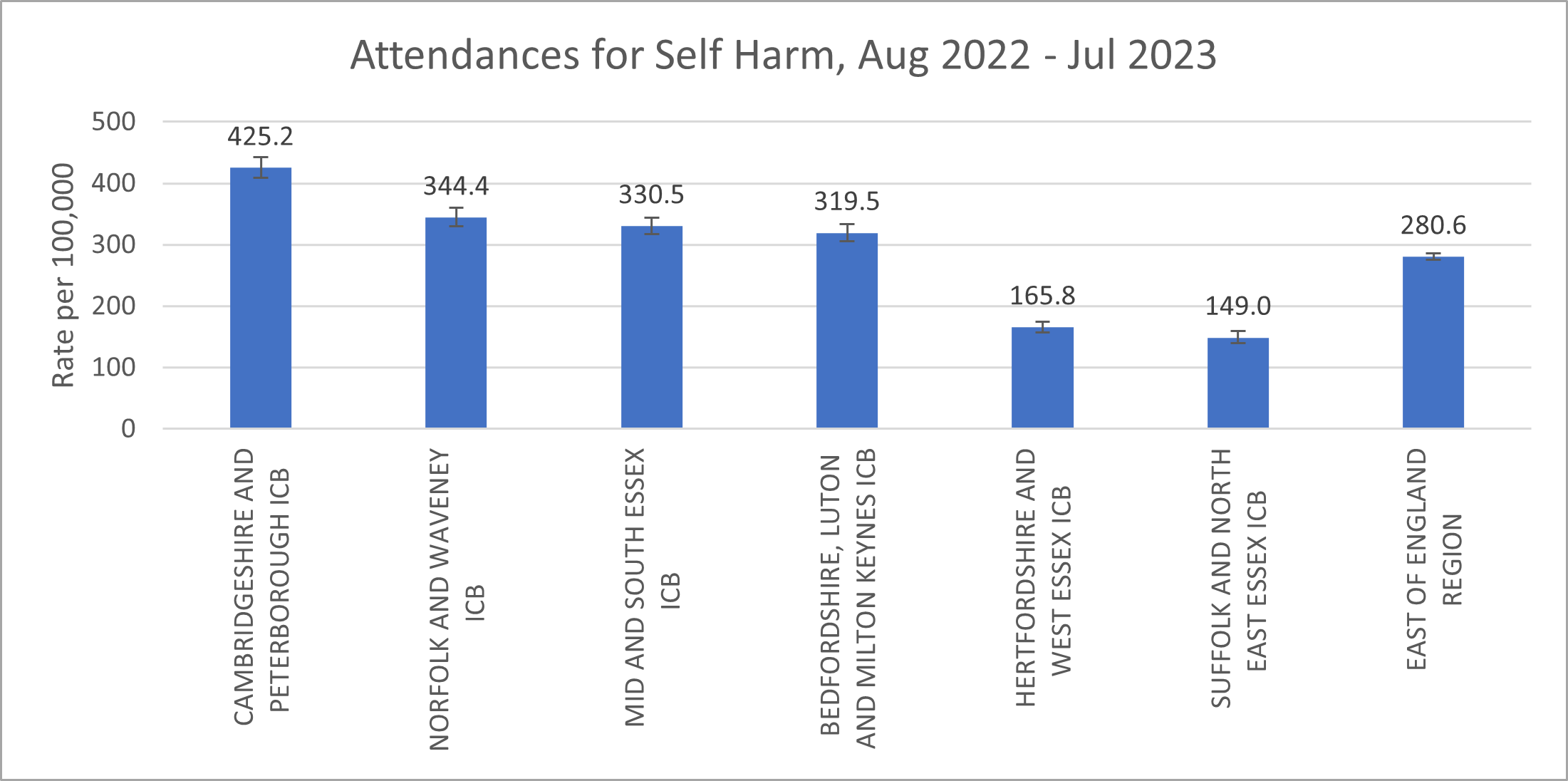
However, attendances for self-harm appear to be higher in Cambridgeshire and Peterborough than other areas. This may be due to the coding practices of hospitals for self-harm, as highlighted by a recent report by Fullscope, which focused on self-harm amongst children and young people in Cambridgeshire and Peterborough. Another potential contributing factor is that Cambridge University Hospitals NHS Foundation Trust (Addenbrooke’s Hospital) is the trauma centre for the East of England, so receives people from across the region for trauma care.
Figure 40: Accident and Emergency attendances for self-harm, Cambridgeshire and Peterborough ICS, August 2022 – July 2023. Source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
How long do people spend in Accident and Emergency?
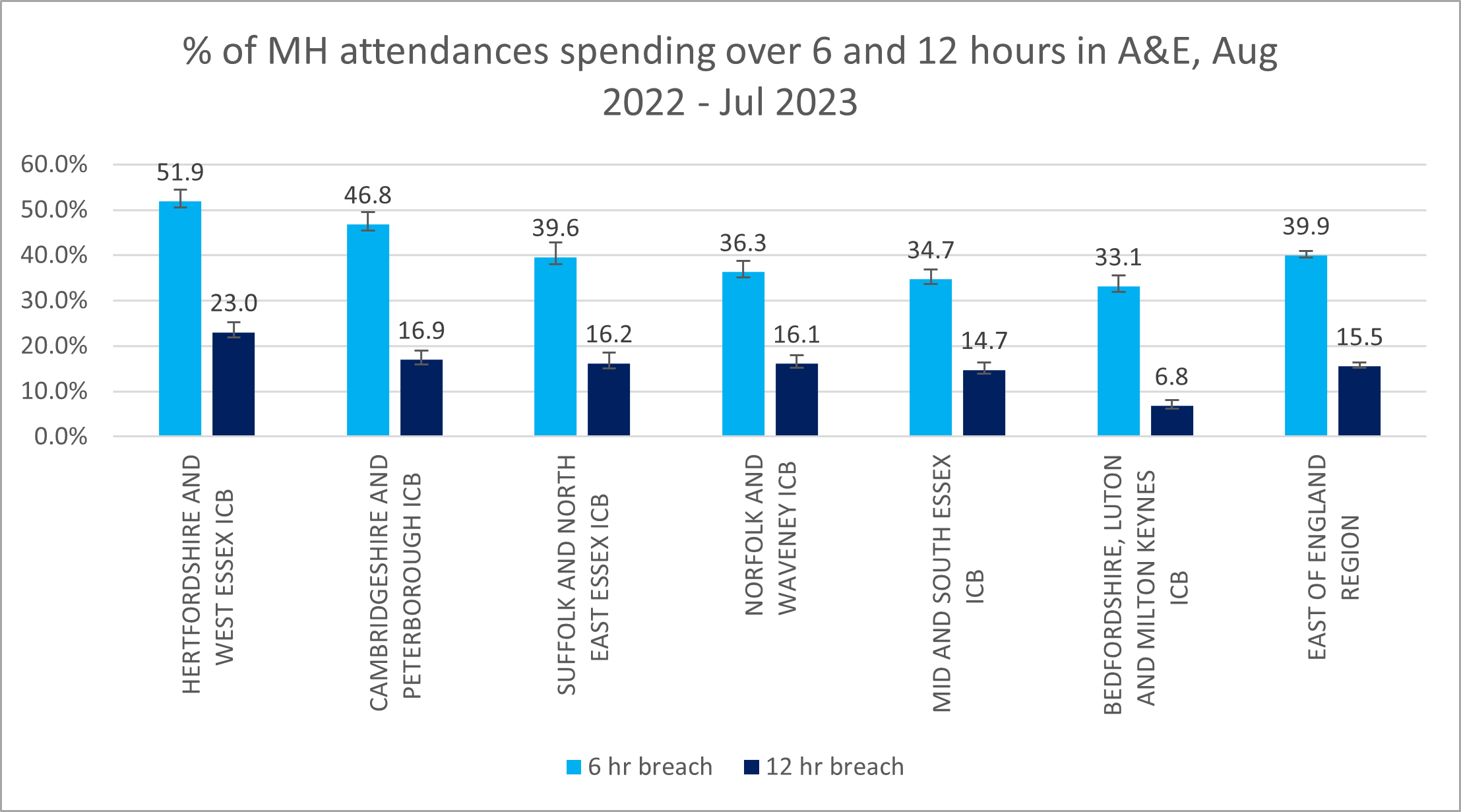
- Over the past couple of years, an increasing proportion of people attending Accident and Emergency for reasons relating to mental health in Cambridgeshire and Peterborough have ended up spending over 6 or 12 hours in this department.
- For people attending Accident and Emergency for mental health related reasons between August 2022 and July 2023:
- Almost half (47%) of spent over 6 hours in this department.
- Around 1 in 8 (17%) spent over 12 hours in Accident and Emergency. This is higher than most areas in the East of England.
- This is also higher than the length of time people spent in Accident and Emergency when their chief complaint related to their physical health. 9% of all people attending this service spent more than 4 hours in the Accident and Emergency department in Cambridgeshire and Peterborough in June 2023 (NHS England, 2023c).
Figure 41: Proportion of mental health attendances spending over 6 and 12 hours in Accident and Emergency, Cambridgeshire and Peterborough ICS, August 2022 – July 2023. Data source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
What do people say about this service?
- A national survey carried out in 2014 found that Accident and Emergency departments were felt to be the worst for service user experience, compared to other options in a mental health crisis such as voluntary sector organisations, GPs and community mental health teams (Care Quality Commission, 2015). Fewer than 1 in 3 people reported that the advice and support they got was ‘right for them’ (Care Quality Commission, 2015).
- International studies highlight that people attending Accident and Emergency in mental health crisis often have poor and stressful experiences, due to staff attitudes, waiting times and the environment of this setting, which can be distressing in itself (Sacre et al., 2022).
Liaison psychiatry services
Liaison psychiatry services provide psychiatric assessment and treatment to patients who may be experiencing mental ill health whilst in general hospital wards (such as Emergency Departments and inpatient wards) (Public Health England, 2019). They provide support for people who present with both physical and mental health symptoms. National studies show that these services improve quality of care, reduce the length of time people stay in hospital and reduce the risk of adverse events linked to mental health (Royal College of Psychiatrists, 2013).
The key trends in referrals to liaison psychiatry for working-age adults (aged between 18 and 65) are:
- Addenbrooke’s: referrals to liaison psychiatry have increased steadily since 2016.
- Hinchingbrooke Hospital: referrals to liaison psychiatry seem relatively stable since 2021.
- Peterborough Hospital: referrals to liaison psychiatry seem relatively stable since 2021.
How many people are referred to this service?
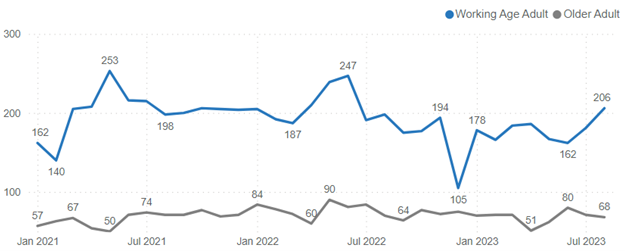
Referrals to liaison psychiatry in Peterborough City Hospital seem relatively stable since 2021. Data was not collected on this system before then.
Figure 42: Referrals to Liaison psychiatry in Peterborough City Hospital, January 2021 – July 2023.
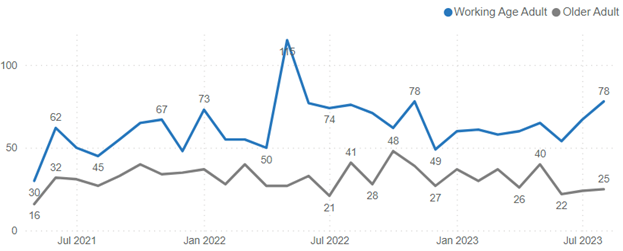
Referrals to liaison psychiatry in Hinchingbrooke Hospital peaked in May 2022, but have otherwise remained relatively stable since 2021.
Figure 43: Referrals to Liaison psychiatry in Hinchingbrooke Hospital, May 2021 – August 2023.
Referrals to liaison psychiatry in Cambridgeshire South have increased steadily since 2016. There was a noticeable decrease in referrals in 2020, when NHS Trusts were asked to urgently discharge any hospital inpatients who were medically fit to leave hospital to increase capacity in response to the COVID-19 pandemic (Nuffield Trust, 2023). Note that data is divided differently on this system, with a separate category for referrals relating to substance misuse.
Figure 44: Referrals to liaison psychiatry, Cambridgeshire South (Addenbrooke’s and the Rosie Hospital), 2014 – 2022. Data source: Epic
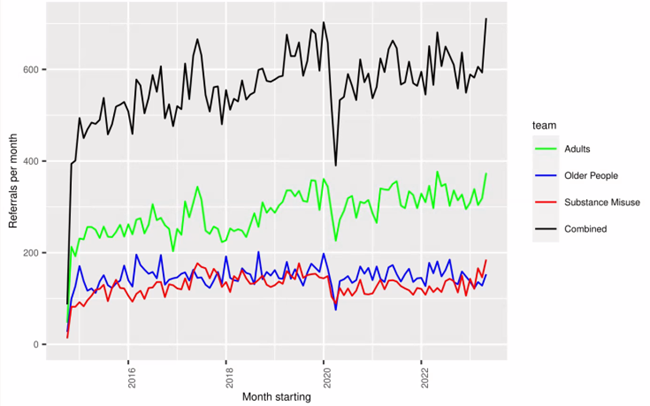
Note: the initial low figures in 2014 are an artefact of moving from paper to electronic systems.
Where are people referred from?
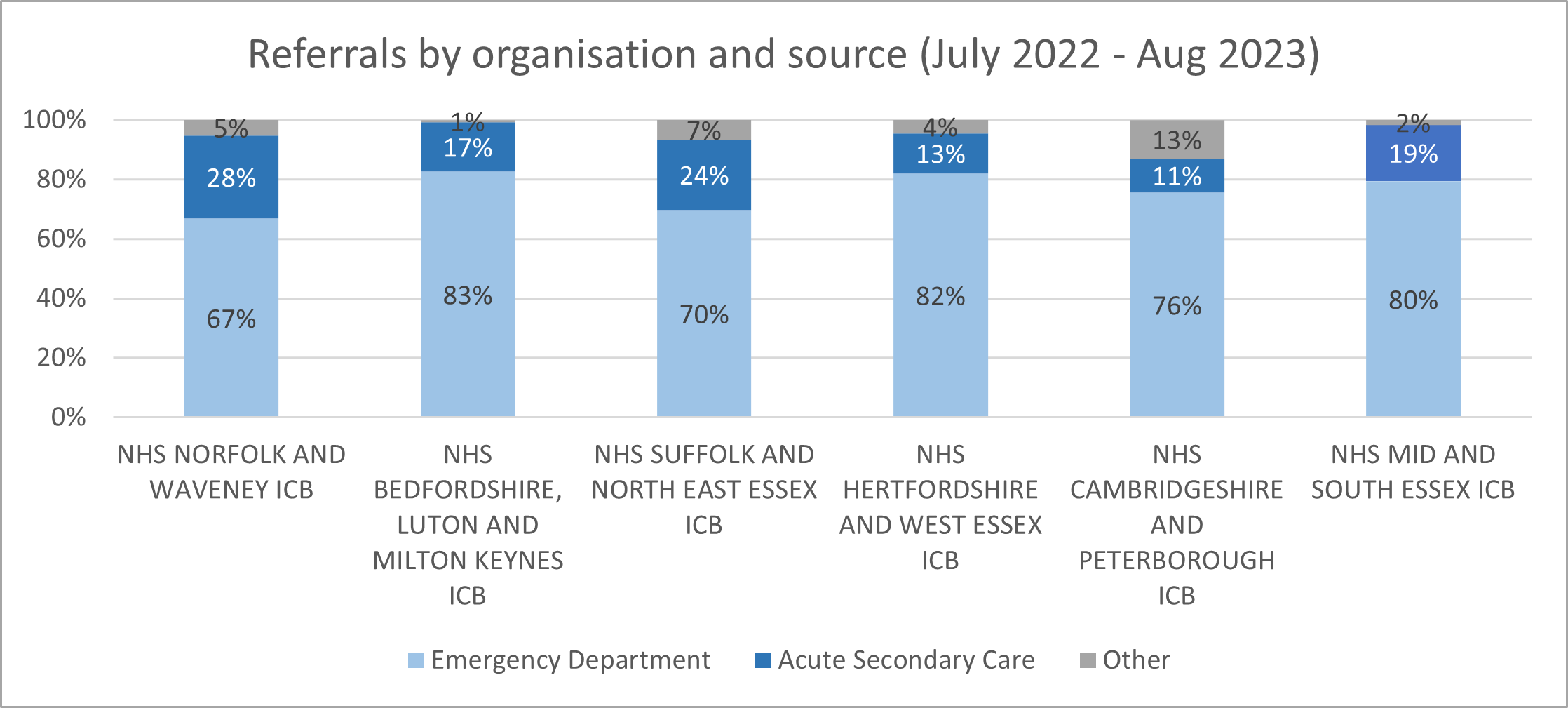
Over the past year (July 2022 to August 2023), three quarters (76%) of referrals to liaison psychiatry teams in Cambridgeshire and Peterborough have been from the Accident and Emergency (Emergency Department). Compared to recent years, there were increasing levels of referrals from the Accident and Emergency, but lower levels of referrals from acute wards.
Figure 45: Referrals to Liaison Psychiatry by organisation and source, 18 – 64 years, Cambridgeshire and Peterborough ICS, July 2022 – August 2023. Data source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
What is the response time for this service?
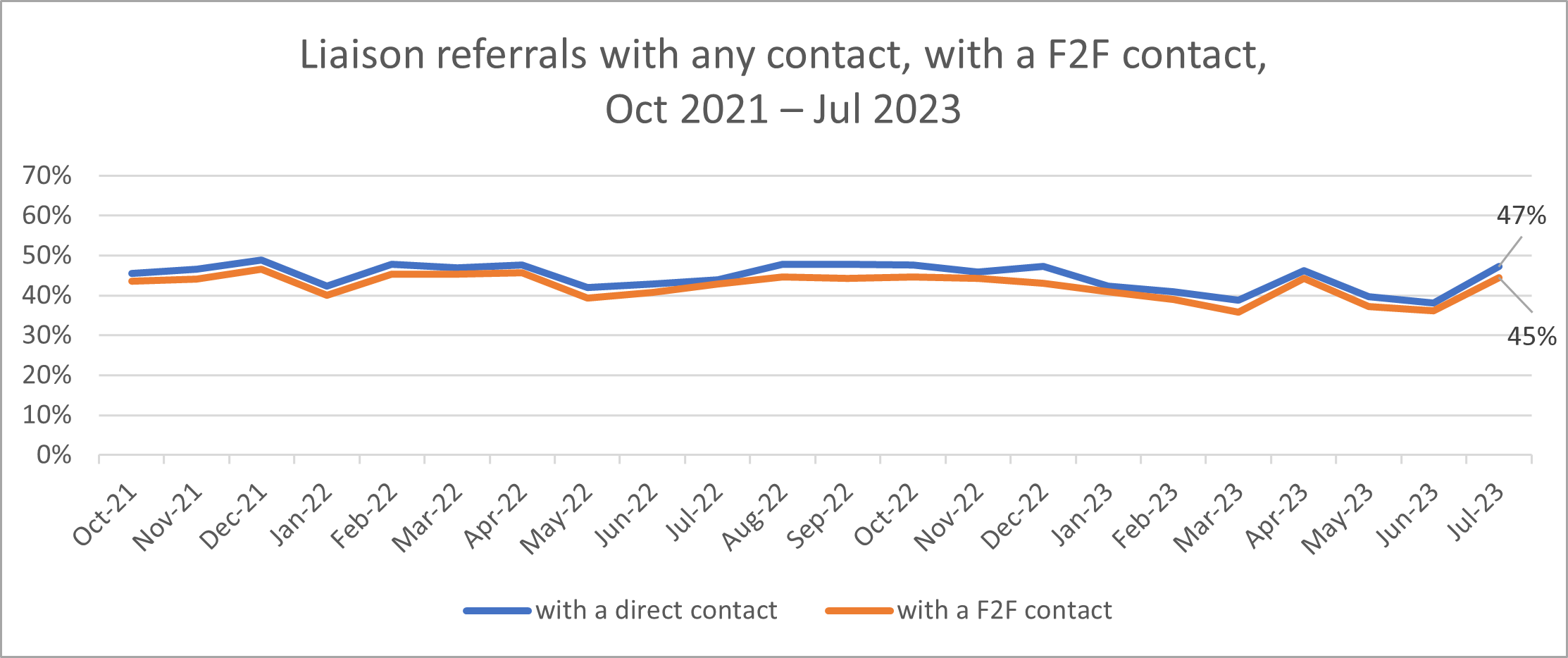
In Cambridgeshire and Peterborough ICS, the proportion of liaison referrals with any contact and face-to-face contact has shown relatively stable trends since October 2021.
Figure 46: Referrals to Liaison Psychiatry with any contact and with a face-to-face (F2F) contact, 18 – 64 years, Cambridgeshire and Peterborough ICS, October 2021 – August 2023. Data source: Urgent and Emergency Mental Health Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
How do local services compare to national standards?
In 2022/23 (NHS England, 2023h):
- 2 out of 3 local acute hospitals met the ‘core 24’ service standard, which sets out a range of support and responses on a 24 hour basis (such as the availability of consultant psychiatrists).
- 2 out of 3 mental health liaison teams were open 24/7.
Police
Some people experiencing mental health crisis come into contact with police. There are a range of local strategies and approaches aiming that this group receives the most appropriate mental health support.
Integrated Mental Health Team
- The Integrated Mental Health Team (IMHT) are specialist mental health staff based at the police force control room in Hinchingbrooke. They work to ensure the most appropriate pathways are taken for individuals in mental health crisis.
- This team supports people in mental health crisis; gives support to the police whilst liaising with mental health teams in relation to police matters; supports police on help with missing persons and domestic abuse cases; and advises operations and gives clarity to officers over the Mental Health Act.
Police and Mental Health Response Car
The Police and Mental Health Joint Response Cars (PMHJRC) aim to improve support for patients in mental health crisis, by exploring options of care within the community. These cars are staffed by two police constable and one Band 7 mental health practitioner; and respond mental health crisis and concern for person calls. The aims of this service are:
- To provide patients in a mental health crisis with a specialist resource that meets their presenting needs.
- To reduce the number of detentions under Section 136 of the Mental Health Act, by identifying and implementing other, more appropriate plans for care.
- To improve the patient and staff experience regarding community-based mental health presentations.
- To improve and promote system working for the benefit of all partners within the locality.
- To reduce the amount of hours police are engaged dealing with mental health crisis.
- To improve the skills police services when dealing with mental health crisis.
There are two mental response cars, one based in the North (MA21) and the other in the South (MA20). From June 2022 to August 2023, the use of Section 136 was avoided on between 60 to 100% of occasions.
Figure 47: Section 136 use in shifts covered by Joint Mental Health Response Cars, June 2022 – August 2023.
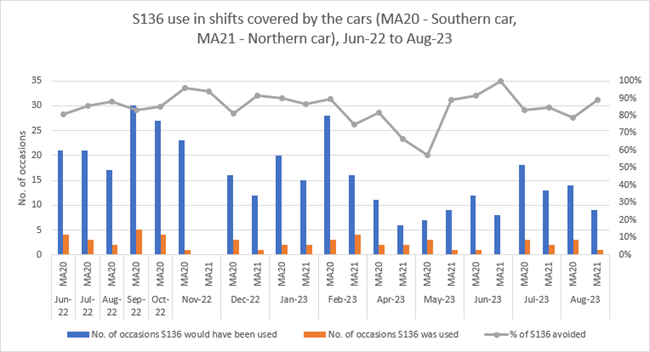
Note that this data only covers the car shifts, not the total number of Section 136 detentions.
Operation Farmington
- Operation Farmington is a project across Cambridgeshire and Peterborough in which multi-agency information sharing is used to aid police decision making when responding to calls for service from those who are “high demand” (either by repeated calls to the Police Service Centre and Force Control Room, Custody or for police attendance in the community)
- It recognises that many people in contact with the criminal justice system (victims, suspects and witnesses) have unmet mental health and/or substance use needs and aims to provide the ‘right care at the right time from the right service’,
Right Care, Right Person
Right Care, Right Person (RCRP) is a national programme ‘designed to ensure that people of all ages, who have health and/or social care needs, are responded to by the right person, with the right skills, training, and experience to best meet their needs’ (96). All police forces are moving towards police officers only attending mental health calls when there is an immediate risk to life or serious harm, or where a crime is involved.
In Cambridgeshire and Peterborough, ‘Concern for Welfare’ calls have been handled under RCRP since the 13th of November 2023.
Mental Health Act
The Mental Health Act is a law that allows people to be sectioned (detained in hospital) if they have a mental health condition and need treatment, and certain conditions are met. There are different types of sections, which have different rules about how long people can be detained (Mind, 2023).
Mental Health Act Assessment Pathway Review 2023
In 2018, reforms were proposed to the Mental Health Act with the aim to better empower patients to make decisions about their care, to improve the experiences of patients from ethnic minority groups and to reduce the use of the Mental Health Act for people with a learning disability and autistic people (Garratt, 2023).
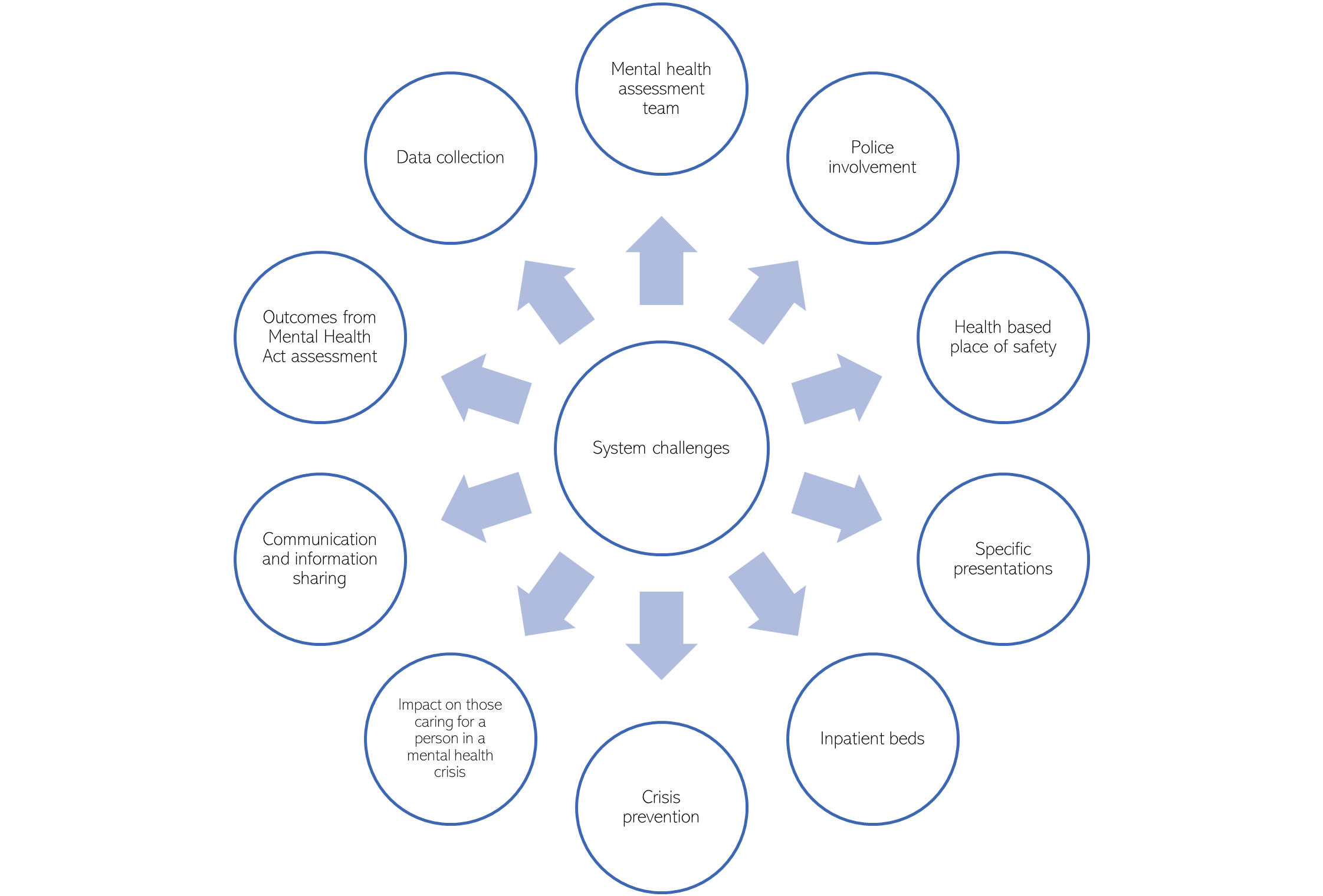
Due to these planned legislative changes, and reports of issues in the Cambridgeshire and Peterborough Mental Health Act ‘pathway’, the system has invested in a multiagency review of the Mental Health Act pathway. This review began with 3 workshops, held between April and June 2023, in which over 60 stakeholders helped to identify system challenges and potential solutions. Workshop participants, including people with lived experience, identified potential solutions which would help resolve these challenges, the prioritised options of which will be developed as a business care.
Figure 48: System challenges identified in the Cambridgeshire and Peterborough Mental Health Act Assessment Pathway Review 2023
What do people say?
A review of international research into the experiences of people assessed and detained under mental health legislation found that (Akther et al., 2019):
- In most studies, a proportion of patients reported that their involuntary admission had helped avert risk and protect them from harm, but some felt that greater provision of timely and appropriate information could help patients feel safer.
- Many people reported that they were not given basic information about this what happened to them and why. When people were provided with clear information, this appeared to reduce fear and the impact of coercion, improve relationships with staff and result in patients feeling less disempowered.
- In the great majority of studies, patients described wanting to be involved in decisions about their care. Good relationships with staff could facilitate involvement in decision making. Carers’ input to decisions was appreciated particularly when patients were too distressed to engage, but this could also leave patients feeling excluded from decision-making.
As part of the Cambridgeshire and Peterborough Mental Health Act Assessment Pathway Review (2023), people with lived experience of the pathway (including as carers) highlighted that:
- Local practice is that requests for planned Mental Health Act assessments are not completed if a bed has not been identified. This leads to delays which may increase distress and anxiety for the individual and their carers, and may also increase the use of Section 136 detentions as people reach ‘crisis point’.
- The process of carrying out Section 135, which requires a warrant application, takes long time. This can cause considerable distress and trauma to both the individual and those that they live, due to having to maintain the safety of the individual whilst the process is completed.
- The use of restraint to maintain the safety of the individual and others as part of the assessment process was raised as a concern, due the long-term impacts this can have on the individual and their loved ones.
- As the only Section 136 Suite in the county is based in Fulbourn, people living in the North of the county do not have equitable access to services and find it difficult to be supported by friends and family.
- In 2022/23 64% of those detained under Section 136 of the Mental Health Act were initially conveyed for assessment to their local Accident and Emergency department. People identified concerns that this is not the ‘best’ place for a person to be assessed and this related to:
- Limited or no private space for the assessment to be conducted, thus impacting on the dignity and privacy of the individual.
- That maintaining the individual’s and other safety in this environment was more complex and would often mean that either police or security staff would be seen to be ‘on guard’, stigmatising the individual by ‘criminalising’ the assessment process.
- That staff attitudes towards people in mental health crisis could occasionally be unhelpful and led to both the individual being assessed and the staff conducting the assessment feeling unwelcome or discriminated against.
- Specific challenges relating people caring for someone experiencing a mental health crisis were identified:
- Additional sense of responsibility and potential resulting distress and anxiety when supporting a person whilst a Mental Health Act assessment is arranged and/or the delay in the assessment being completed.
- Sense of holding the risk and responsibility for the individual who may present at significant risk to self or others.
- Feeling abandoned and unsupported at the end of the assessment process when the person is not admitted or offered additional help and support.
- Lack of specific carer support prior to, during and after the assessment process.
How many people are detained?
The data below covers uses of the Mental Health Act in CPFT (Cambridgeshire and Peterborough Foundation Trust). It does not over NWAFT (North West Anglia Foundation Trust) or CUH (Cambridge University Hospital).
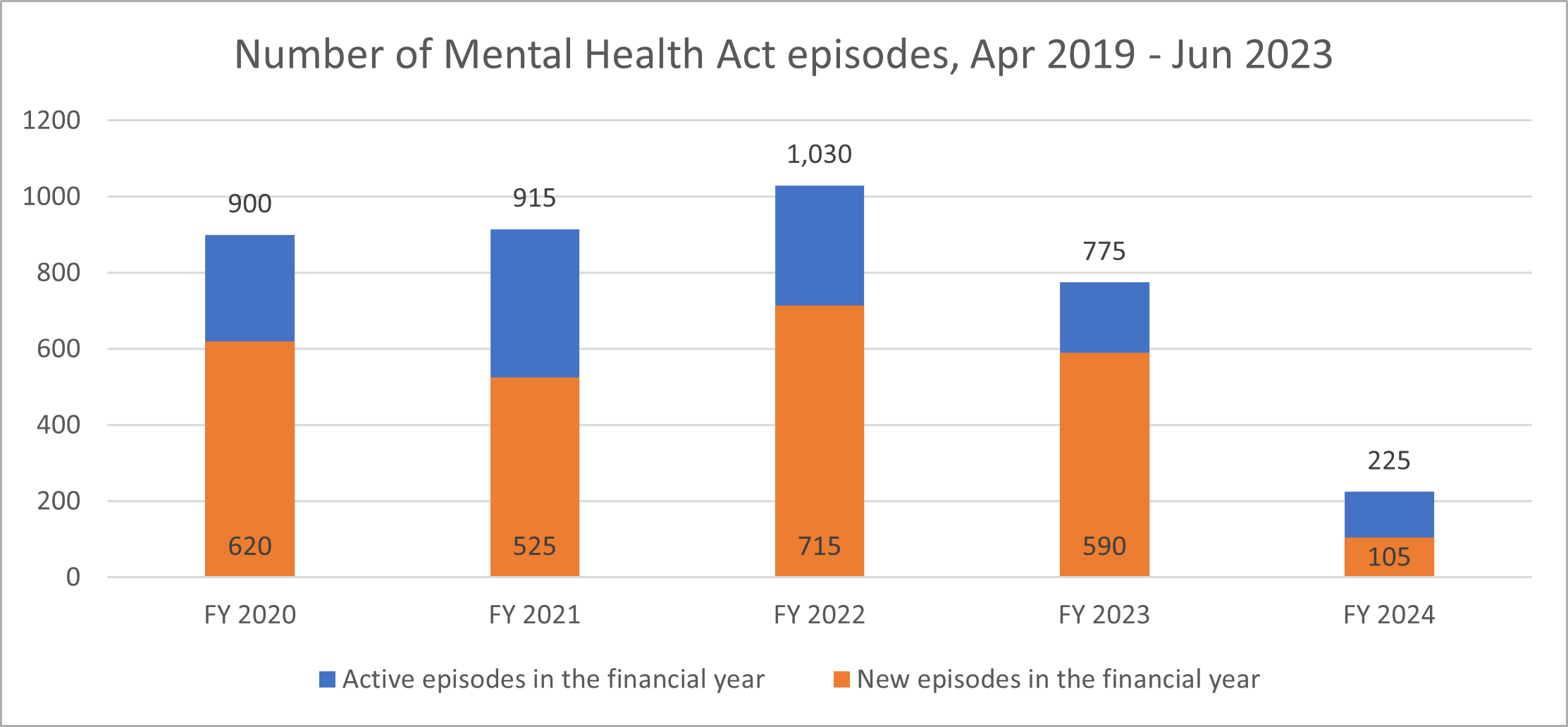
In Cambridgeshire and Peterborough, there was a 25% decline in in the number of Mental Health Act episodes in 2023/24, compared to the previous financial year.
Figure 49: Number of Mental Health Act episodes in Cambridgeshire and Peterborough, April 2019 – June 2023. Data source: MHA Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
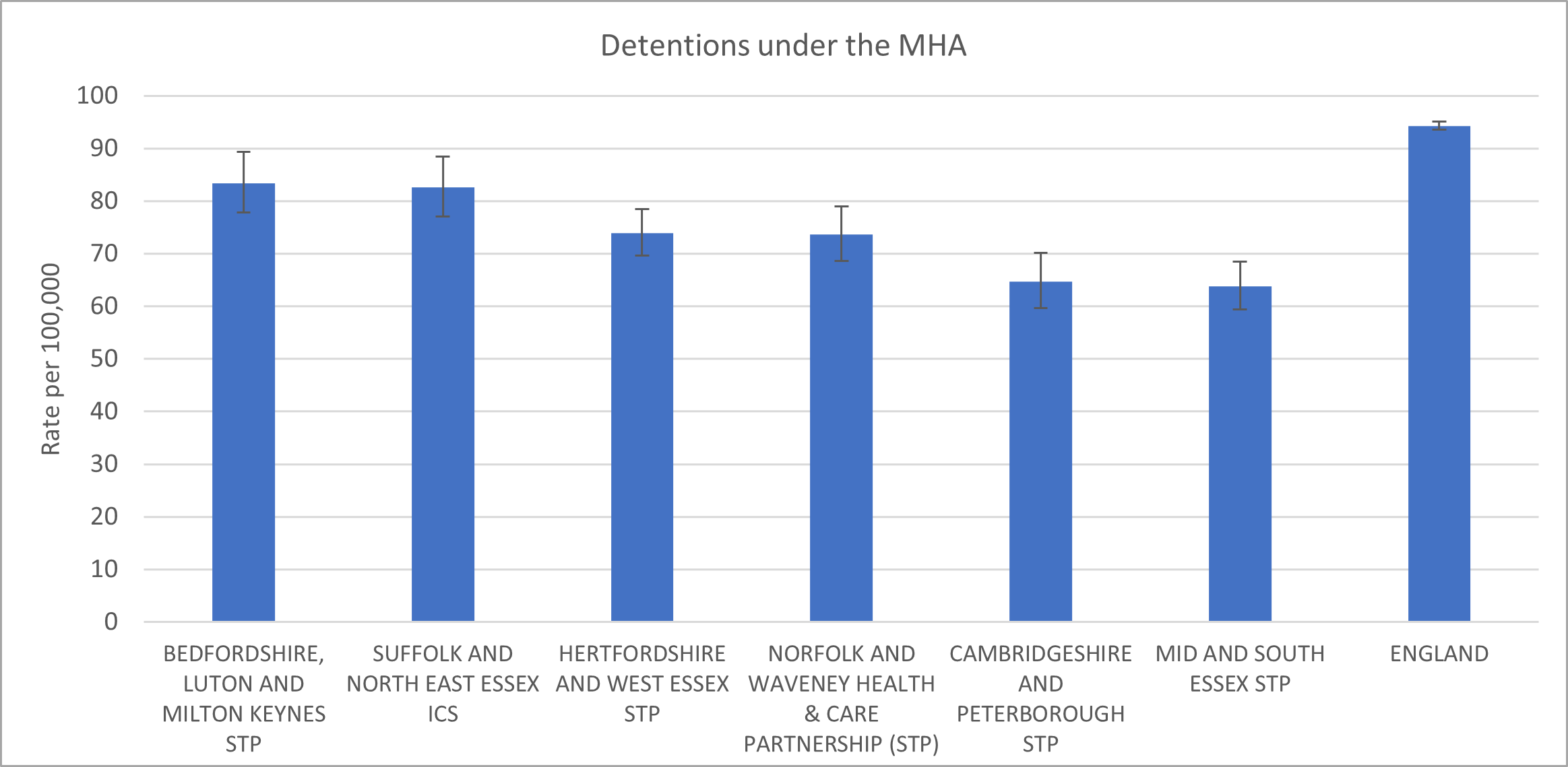
In 2021/22, the rate of detentions under the Mental Health Act was lower in Cambridgeshire and Peterborough compared to most other areas in the East of England.
Figure 50: Rate of detentions under the Mental Health Act per 100,000 of the total population by STP, East of England, 2021-22. Data source: Mental Health Act Statistics, Annual Figures, 2021-22 – NHS Digital
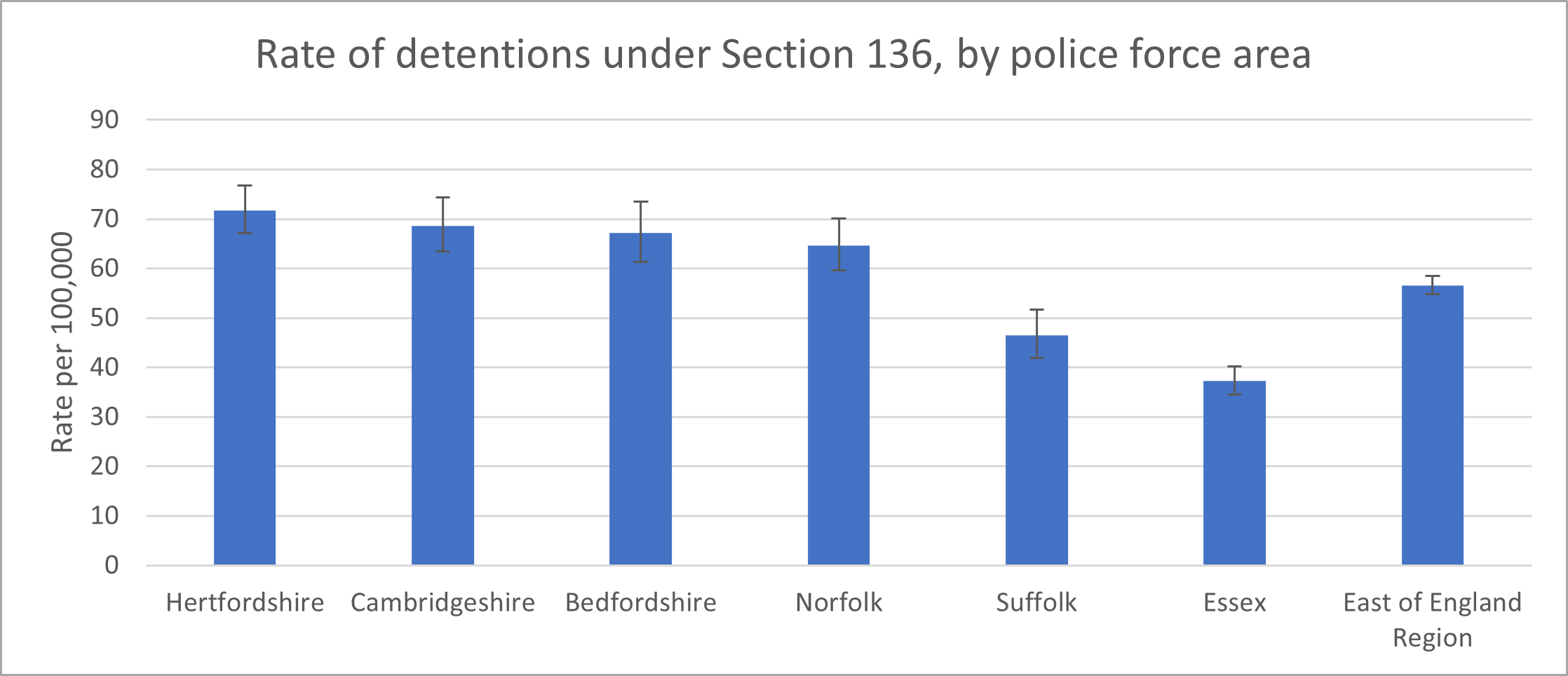
In 2021/22, the rate of detentions under Section 136 per 100,000 population in Cambridgeshire Constabulary (69 per 100,000) was the second highest in the East of England region. It was significantly higher than the regional average of 57 per 100,000.
Figure 51: Rate of Mental Health Act detentions under Section 136, East of England, 2021/22. Data source: Gov.uk
How long are people detained?
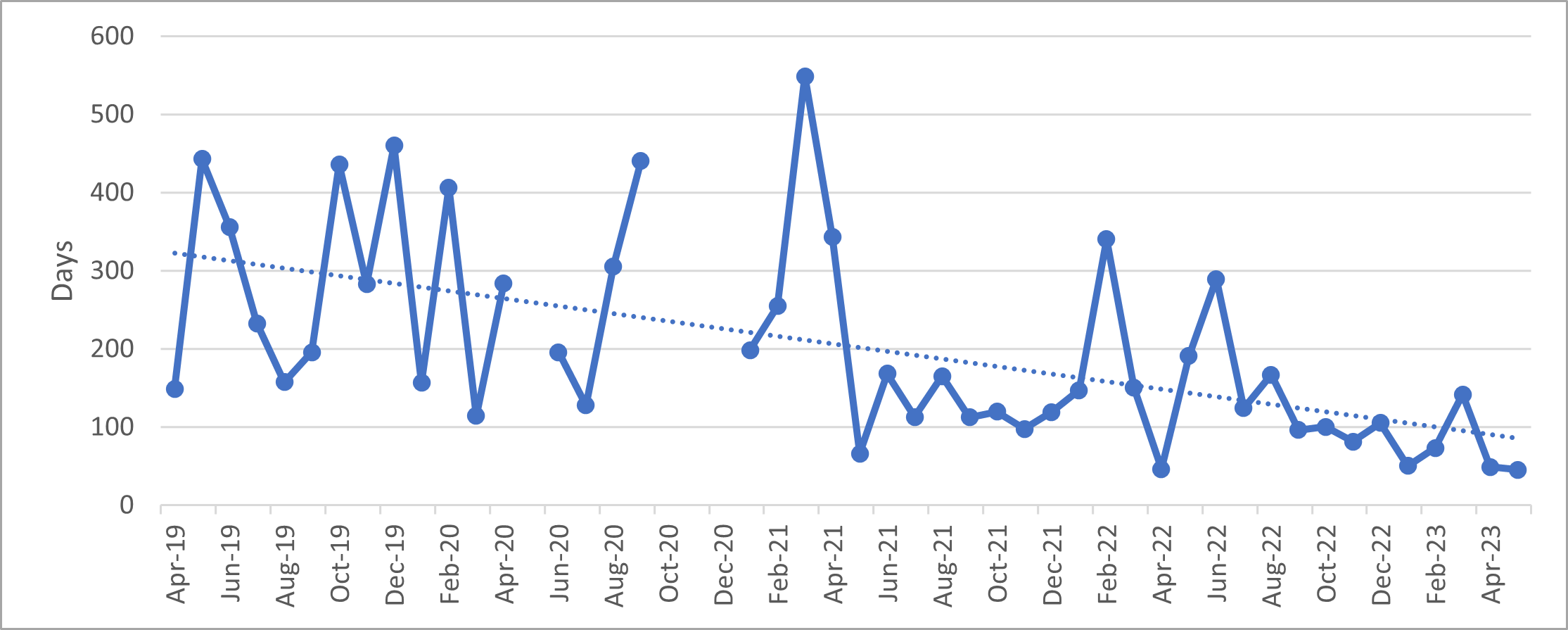
The average length of Section 2 detentions in Cambridgeshire and Peterborough increased from April 2019 to May 2023, from around 15 to 20 days. Contrastingly, a declining trend is seen Section 3 detentions, from an average of 300 to below 100 days.
Figure 52: Average length of MHA episodes (section 2) for adults aged 18 – 64, Cambridgeshire and Peterborough ICS, April 2019 – May 2023. Data source: MHA Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
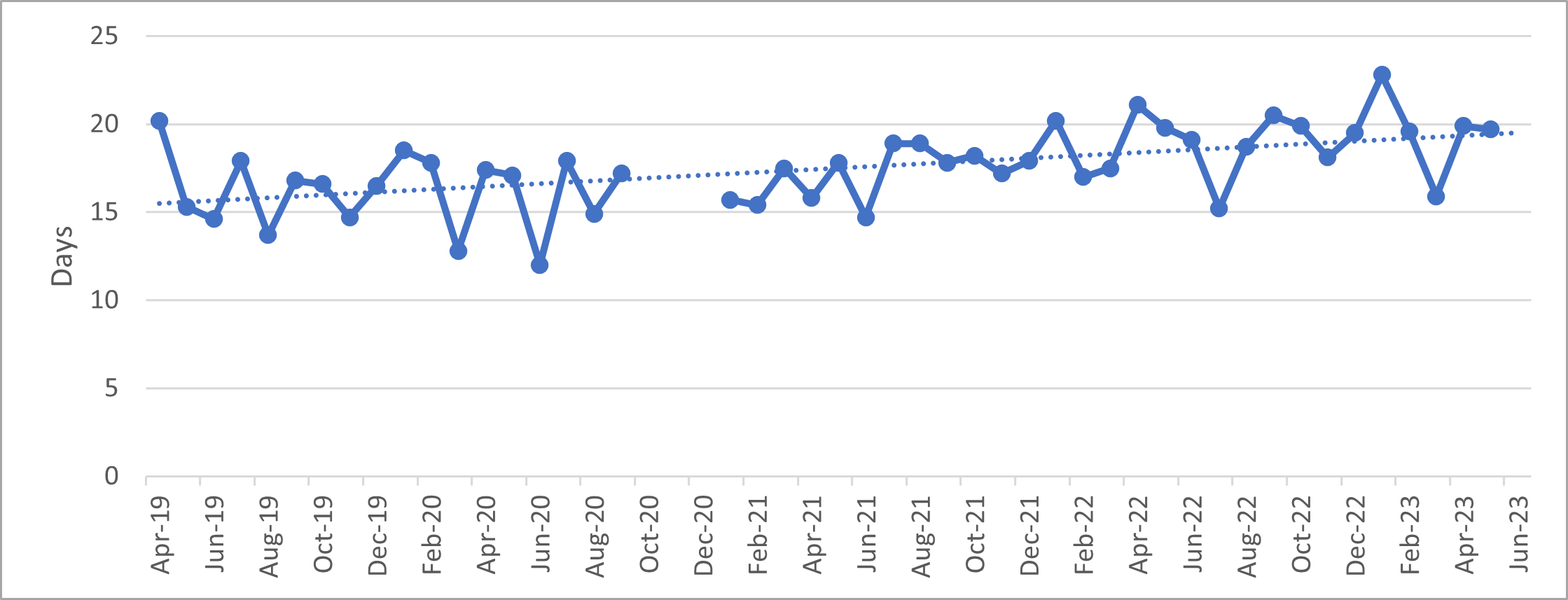
Figure 53: Average length of MHA episodes (section 3) for adults aged 18 – 64, Cambridgeshire and Peterborough ICS, April 2019 – May 2023. Data source: MHA Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
Repeat detentions
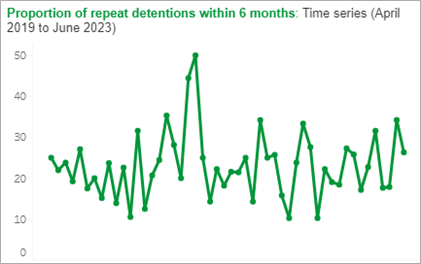
In the past year, an increasing proportion of people have been detained under the Mental Health Act, after having previously been detained in the preceding six months.
Figure 54: The proportion of repeat detentions within 6 months, Cambridgeshire and Peterborough ICS, April 2019 – June 2023. Image source: MHA Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
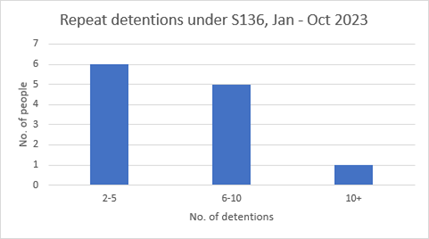
There are a small number of individuals who are detained under Section 136 multiple times. For example, in the 10 months from January to October 2023, 5 people were detained between 6 to 10 times, and one person was detained over 10 times.
Figure 55: Repeat detentions under Section 136, January – October 2023.
Which groups are more likely to be detained by the Mental Health Act?
In the 12 month period ending in June 2023, in Cambridgeshire and Peterborough:
- A similar proportion of men and women were detained under all sections the Mental Health Act. However, men made up 83% of the people detained via the criminal justice system and 70% via community treatment orders.
- 44% of people detained under Section 136 were from the most deprived quintile.
- The proportion of people detained under the Mental Health Act who were from ‘Black’, ‘Mixed’ or ‘Other’ ethnic groups was substantially overrepresented compared to the proportion within the general population.
- 23% of people detained under the Mental Health Act were age 65 or over, although the age breakdowns of people detained varied substantially by the type of section. All the people detained under Section 136 were aged between 18 and 54 years, with a higher proportion among the 35 to 44 age group.
- 11% of all people detained under the Mental Health Act had a learning disability and/or were autistic. About 1 in 5 people detained via the criminal justice system had a learning disability and/or were autistic.
More detailed breakdowns by the type of section can be found here (embed slides). For more information on the national trends in Mental Health Act detentions, see this report (link to slides).
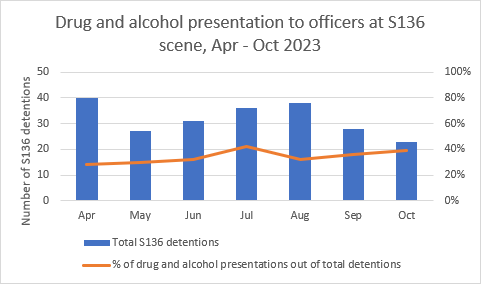
From April to October 2023, 30 to 40% of Section 136 detentions each month were thought to involve drug or alcohol presentations. This means that police officers believed that the individual involved had used drugs and/or alcohol, so may not reflect true figures.
Figure 56: Recorded drug and alcohol presentations by officers at Section 136 scene, April – October 2023.
Voluntary and community sector
There is a range of voluntary and community sector support for people experiencing mental health crisis. Some of the largest organisations offering this support locally are Lifecraft, CPSL Mind and the Samaritans; although there are also a range of helplines run by national organisations.
Lifeline
Lifeline is a ‘free, confidential and anonymous telephone helpline service for people in Cambridgeshire and Peterborough that is currently available from 11am – 11pm every day. Lifeline provides listening support and information to someone experiencing mental distress or if you are supporting someone in distress’ (Lifecraft, 2023b). It is run by Lifecraft (add link). In 2022/23:
- This service took 8,749 calls and was open for 4,015 hours.
- Volunteers offered 2,904 hours of support.
- 710 people called Lifeline for the first time.
- The most common reasons for calling were isolation (19%), anxiety (14%), distress (8%) and depression (7%).
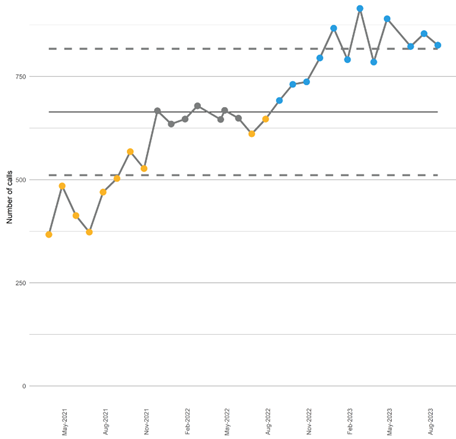
The number of callers to Lifeline has increased from October 2022 to August 2023, but there has not been a significant change in the number of first-time callers over this time. This does not necessarily reflect an increase in mental distress in the population: Lifeline has increased their advertising over this time period, and the number of calls taken by this service is impacted by the number of open lines. However, anecdotal evidence suggests that callers to Lifeline has been more unwell and had more complex experiences of distress.
Figure 57: Number of calls to Lifeline, April 2021 – August 2023
Samaritans
Cambridge Samaritans provides emotional support to anyone in distress. This includes walk in support from 10.30 am to 10pm daily, and telephone and email support (Samaritans, 2023). In 2021, the Cambridge Samaritans branch:
- Answered 26,943 calls.
- Spent 8,452 hours on the phone.
- Sent 1,089 e-mails.
The Sanctuary
CPSL Mind run Sanctuaries in Cambridgeshire and Peterborough. These offer telephone support (between 11am and 5pm) and face-to-face support (6pm to 1am) for people experiencing mental health crisis (CPSL Mind, 2023).
After discharge from crisis services, individuals can be supported by the Discharge Buddy Service. This offers short-term social, practical and emotional support to help recovery and prevent future crisis. This service is open to young people and adults, who are referred via the crisis care pathway and community mental health teams (CPSL Mind, 2023).
Follow up support (Lifecraft)
Lifecraft provides a range of follow-up support for people after discharge from The Sanctuary, after being detained under Section 136 and for those who have been missing from home. In 2022/23:
Sanctuary Aftercare Service
- 1,349 referrals into the service and 877 unique people supported
- 1,129 signposts made
- 70 safety plans created and 12 updated
S136 Follow-up Service
- 51 referrals into the service and 38 people supported
- Over 22 hours of support given
Missing from Home Service
- 74 referrals into the service and 46 people supported
- Over 20 hours of support provided
Additional resources
- The local data packs give an overview of prevalence and service use
- NHS England » Crisis and acute mental health services
- All Age Crisis Care | Royal College of Psychiatrists (rcpsych.ac.uk)
- Mental Health – Adult Crisis and Acute Care GIRFT Programme National Specialty Report
- National Partnership Agreement: Right Care, Right Person
- Right Care Right Person toolkit
- My Crisis PACk (Preferences for Admission, treatment and Care) tool
References
Full list of references is included at the end of this chapter.