Interventions for severe mental illness
- Severe mental illnesses are long-term mental health conditions that have a substantial impact over multiple aspects of people’s lives (Swinson et al., 2016). This term is commonly used to describe bipolar disorder and psychotic disorders, but can also include other mental health conditions when the impact is severe such as anxiety, depression, and eating disorders (Swinson et al., 2016).
- In NHS guidance on physical health checks, severe mental illness (SMI) is defined as a recorded diagnosis of bipolar affective disorder, schizophrenia or any long-term psychotic illness (NHS England, 2018b), although people in ‘remission’ are excluded from this register. This definition is used because of the cardiometabolic risks associated with antipsychotics; rather than implying that other mental health conditions are not ‘serious’ or ‘severe’, or do not have their own physical health risks (NHS England, 2018b).
- Community mental health services are ‘secondary care services designed for those with severe mental health conditions (inclusive of psychosis, eating disorders, and bipolar mood disorder), enabling people to access specialised care as close to their home as possible’ (Bagri, 2023).
- This section covers the support offered to people with severe and enduring mental illness, including from primary care, community mental health services, crisis services and voluntary and community sector services. Practical and social interventions are covered here.
Evidence-based interventions
- Community based mental health services support people with mental health conditions in their journey from referral to longer term recovery (Public Health England, 2019). Services should be commissioned to consistently provide rapid access to a full NICE-recommended package of care, delivered in a person-centred and values-based way.
- This includes (National Institute for Health and Care Excellence, 2011; NHS England, 2023d; NICE, 2014):
- person-centred and co-produced approaches to care planning.
- psychosocial and psychological therapy interventions for individuals and their families.
- optimisation of medication and regular medication review.
- physical health assessments and required interventions, including dental and ophthalmologic and healthy lifestyle promotion.
- effective recovery and rehabilitation in home and community settings including support with finding and maintaining stable housing, employment, financial wellbeing and social networks.
- Services should help people achieve and maintain recovery by (Public Health England, 2019):
- providing rapid referral for assessment and secondary care treatment and support where required.
- providing enhanced primary care step-down support to maintain recovery following discharge from secondary mental health services.
- Providing rapid access to care to enable service users to step-up their care as required or self-refer for reassessment.
- routinely recording and publishing patient and carer experience and outcome measures.
Antipsychotics
- Antipsychotics are medications used to reduce and control psychotic symptoms, such as delusions and hallucinations.
- The different types of antipsychotics are sometimes categorised as ‘first-generation’ and ‘second-generation’. Their side effects vary, so the choice of medication is related to an individual’s particular needs.
- Clozapine is a second-generation antipsychotic that is unusually effective but also has particular side effects, so is considered separately below (NICE, 2014).
Clozapine
- NICE guidelines state that clozapine is the only medication known to reduce symptoms and risk of relapse for adults whose schizophrenia has not responded to conventional antipsychotic drugs (National Collaborating Centre for Mental Health, 2014). Around half of people with treatment-resistant schizophrenia respond to clozapine (53).
- Research suggests that fewer than 1 in 3 patients with treatment-resistant schizophrenia receive clozapine in the UK (Whiskey et al., 2021), highlighting unmet need.
- The Clozapine Clinic is a service run by CPFT (Cambridgeshire and Peterborough NHS Foundation Trust) which monitors the effects of clozapine. This includes mandatory blood monitoring (carried out weekly, fortnightly or monthly) and biannual physical health checks.
- The table below demonstrates the potential gap for the use of clozapine within our local area, with a total of 277 people living with treatment-resistant schizophrenia who may benefit from clozapine initiation.
Table 1: Estimated level of unmet need in clozapine treatment in Cambridgeshire and Peterborough, December 2023
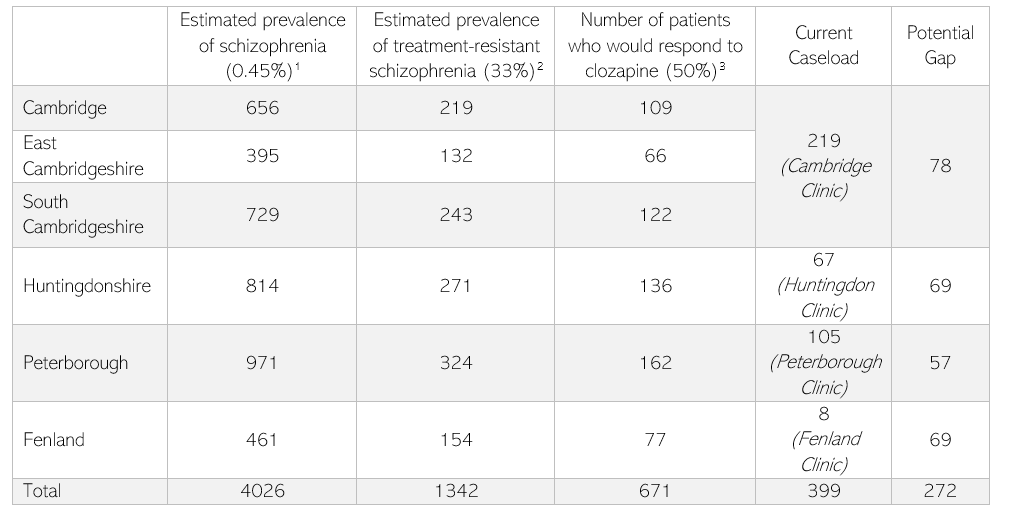
Note that crude estimates for the prevalence of schizophrenia used 2021 Census data and did not account for age, deprivation or rurality. Data sources for estimates:
- Census 2021 and NICE Guidelines (2014) (https://www.nice.org.uk/guidance/cg178/evidence/full-guideline-490503565) [point prevalence]
- Clinical Guidance on the Identification and Management of treatment-resistant schizophrenia (2019) (https://www.psychiatrist.com/jcp/psychiatry/clinical-guidance-on-treatment-resistant-schizophrenia/#:~:text=Treatment%2Dresistant%20schizophrenia%20(TRS),inconsistent%20and%20not%20evidence%20based)
- Mizuno Y, McCutcheon RA, Brugger SP, Howes OD. Heterogeneity and efficacy of antipsychotic treatment for schizophrenia with or without treatment resistance: a meta-analysis. Neuropsychopharmacology 2020; 45: 622–31.
Who is prescribed antipsychotics?
- The majority of people prescribed antipsychotics have been diagnosed with a psychotic illness, bipolar disorder or schizophrenia (Marston et al., 2014). This group meet criteria for the general practice severe mental illness (SMI) register and therefore are offered annual physical health checks, to monitor potential cardiometabolic side effects associated with antipsychotics (add link).
- NICE guidelines also recommend that certain antipsychotics can be used to augment therapy for depression (NICE, 2022a) or to manage delirium in some people receiving palliative care (National Institute for Health and Care Excellence, 2015).
- There is also a cohort of people prescribed antipsychotics who do not meet these criteria. In 2021/22, across England (46):
- 5% of people without a learning disability, who did not have a SMI diagnosis or require palliative care, were treated with antipsychotics.
- 1% of people with a learning disability, who did not have a SMI diagnosis or require palliative care, were treated with antipsychotics.
- National research highlights that people with dementia make up a substantial proportion of this group (Marston et al., 2014), and that a quarter of people with a ‘personality disorder’ diagnosis, with no recorded SMI diagnosis, are prescribed antipsychotics (Hardoon et al., 2022).
- Local guidance in Cambridgeshire and Peterborough highlights that all patients prescribed antipsychotics, including those not on the SMI register, should also receive physical health checks.
References
Full list of references is included at the end of this chapter.