Primary care support for severe mental illness
Primary care works in partnership with secondary care community mental health provision to provide long-term support for people with enduring mental health conditions. The aspiration is that local people can access the right level of care, from the right place, at the right time.
- The Stepped Care Model of Community Mental Health aims to move away from mental health support being delivered either by primary or by secondary care, into a model built around Integrated Neighbourhoods and Primary Care Networks (PCNs). Investment has been made into liaison roles that join primary care, secondary care, voluntary and community sector organisations, as well as in filling gaps in support between Talking Therapies and community mental health services.
- Primary care also provides physical healthcare for people with severe and enduring mental illness, including physical health checks (Royal College of General Practitioners, 2017).
Peterborough Exemplar (2019 – 2022)
- Peterborough was chosen as the site of a two-year NHS England-funded pilot to transform the delivery of mental health support. Prior to the this, feedback to the SUN (Service User Network) highlighted that people felt that they were ‘bounced around’ different services and that often help was only available when they became ‘unwell enough to hit… threshold’
- The Peterborough Exemplar aimed to provide a sustainable, person-centred system of mental health care for Peterborough, which would deliver a better access to a broader range of care options, reduce demand for high-level interventions, give greater service efficiency, and improve patient experience and outcomes.
- Changes introduced as part of the Exemplar include: increasing the number of clinicians and multi-disciplinary staff within CPFT’s Primary Care Mental Health Services (PCMHS), specific mental health clinical leads for each primary care network (PCN), the introduction of a new group programme for people identifying with traits of personality disorder and the dual diagnosis outreach team (DDOT) and the creation of a digital and community engagement team connecting community assets with clinical care.
Improvements as a result of the Peterborough Exemplar include:
- Enhanced professional relationships and partnership working between primary care, mental health specialists, local authorities and the voluntary and community sector.
- Reduced waiting times and increased attended contacts, compared to comparator sites.
- Two new psychology-driven services accessed directly from primary care. These services fill gaps and enhance access for those that had not previously reached specialist mental health service thresholds.
- Support to address social factors through new workers and better use of community assets.
- Increased focus on underserved populations from diverse ethnic groups.
- Focus on prevention and mental wellbeing using a digital approach, supported by a community engagement team.
The Peterborough model has not simply been replicated across the county as each neighbourhood is has unique local needs. However, each neighbourhood across the county now benefits from:
- A dedicated Mental Health Liaison Practitioner within CPFT’s Primary Care Mental Health Service (PCMHS), the support of an Advanced Nurse Practitioner and the offer of a Primary Care Network (PCN) Mental Health Lead GP role, to directly support the PCN Clinical Director and become the key link between primary and secondary care for that set of general practices.
- PCN Mental Health Leads are brought together for a quarterly networking and training session, allowing them to share expertise with peers.
- The How Are You Digital and Community Engagement team work closely alongside Integrated Neighbourhood colleagues, supporting both voluntary and community sector organisations and statutory teams with knowledge of local assets and a website resource that proactively seeks to remove barriers to accessing support.
- Community and clinical expertise being brough together in new Neighbourhood Mental Health Hubs, which provide a space for professionals to reflect, share case studies and exchange information and updates with everyone supporting those with mental health challenges across the neighbourhood, whatever organisation they work or volunteer with.
Primary care mental health service
- CPFT’s Primary Care Mental Health Service (PCMHS, previously known as PRISM) provides specialist mental health support for anyone between age 17 and 65 in Cambridgeshire and Peterborough.
- The PCMHS supports GPs in the provision of person-centred care that considers mental health, physical health and social care needs (Cambridgeshire and Peterborough NHS Foundation Trust, 2023b):
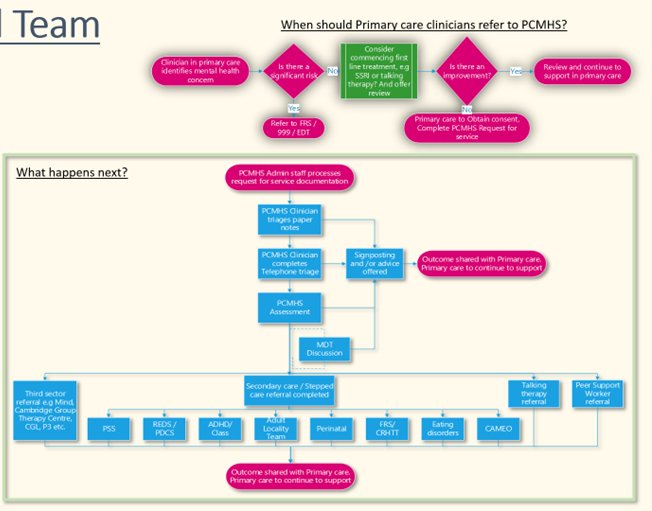
- If a GP identifies a mental health concern, and there is not significant risk that would indicate a crisis pathway needed, they would initially consider a first line treatment as per NICE guidelines, such as Talking Therapies.
- If no improvement is seen and the patient is felt to need support beyond the primary care team (including personalised care roles such as social prescribers), the GP requests service from PCMHS.
- The PCMHS team then triages the patient notes, pulling together a detailed history and complete a telephone triage with the patient if appropriate. This is used to determine if an assessment is in the patient’s best interest, and next steps are then decided, often as part of an multidisciplinary team discussion.
- Supported offered by PCMHS includes mental health assessments, brief interventions, advice on treatment and referrals or signposting to community support (Cambridgeshire and Peterborough NHS Foundation Trust, 2023b). Peer support workers, who have lived or living experiences of mental health challenges, can provide a supportive relationship for people accessing this service (Cambridgeshire and Peterborough NHS Foundation Trust, 2023b).
- PCMHS consists of three teams: a north team covering the Peterborough PCNs, the central team supporting Huntingdonshire and Fenland PCNs, and the south team who cover East Cambridgeshire, South Cambridgeshire and Cambridge City PCNs.
Figure 1: Pathway into the Primary Care Mental Health Service (PCMHS)
Who uses this service?
The number of referrals to the PCMHS has been increasing steadily since June 2020. Before this time period, the COVID-19 pandemic meant that there was a substantial drop in referral numbers.
Figure 2: Total number of unique referrals accessing PCMHS by month, January 2019 – July 2023.
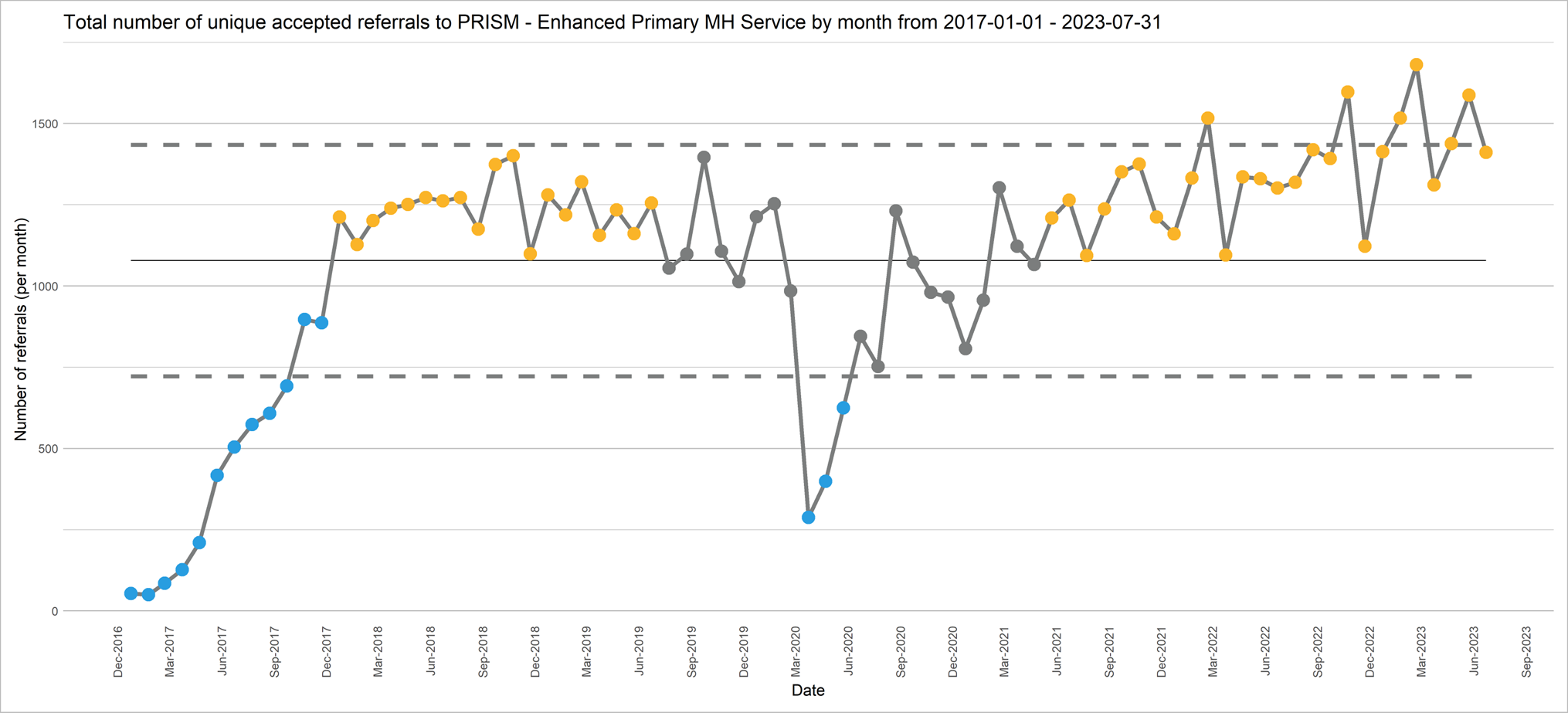
Note that unique referrals are not unique service users: a single individual may be referred to the same service multiple times.
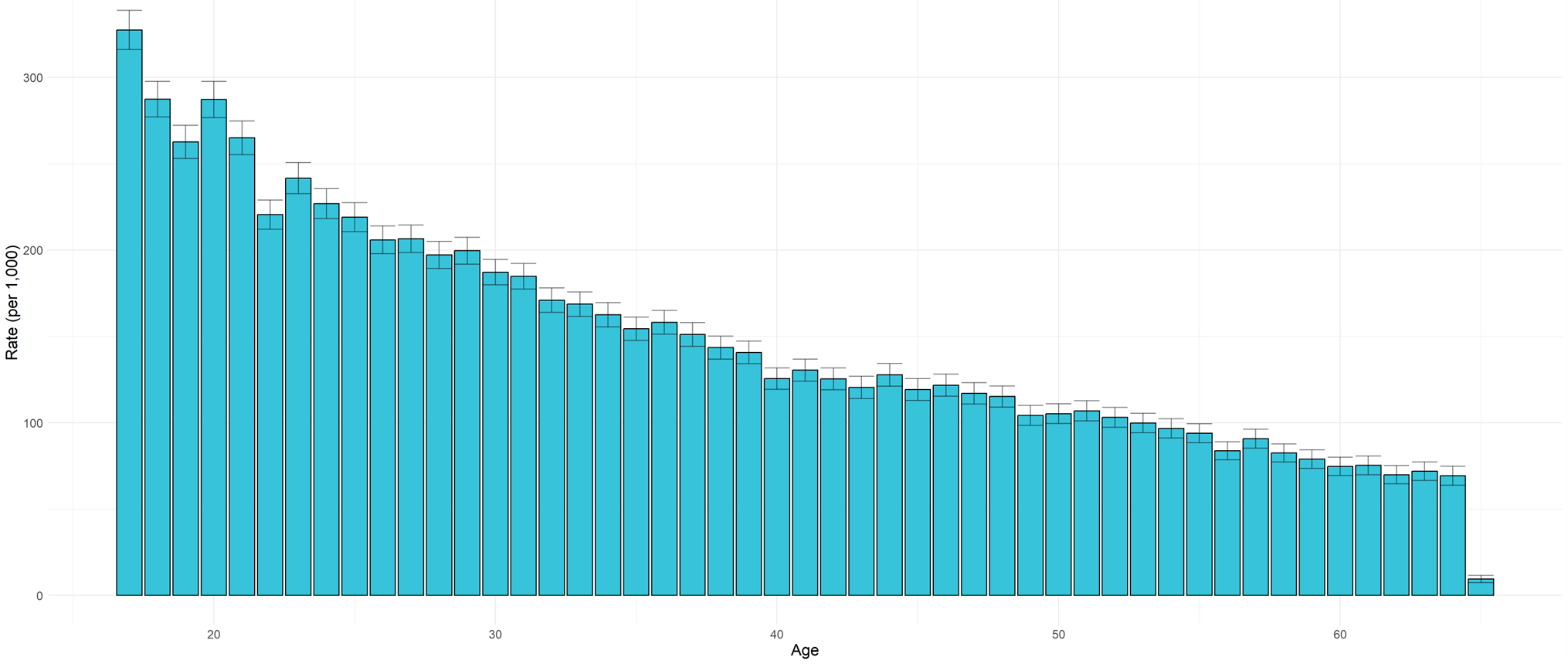
Access rates to the PCMHS decreases by age, with young adults aged between 17 and 21 being most likely to access this service. No adults over the age of 65 were referred to this service from January 2019 – July 2023.
Figure 3: Rate of unique referrals accessing PCMHS by age per 1,000 in the general population, January 2019 – July 2023.
- Women are significantly more likely to access the PCMHS than men.
- Across all age groups, people from more deprived areas are significantly more likely to be referred to and be accepted by the PCMHS.
- People from ‘white’ ethnic groups are significantly more likely to access this service than those from other ethnic groups. There does not seem to significant different in the rate of referrals for people from ‘Black or Black British’, ‘Asian or Asian British’ and ‘Other’ ethnic groups, though these figures may mask differences within these diverse groups.
Figure 4: Rate of unique referrals accessing PCMHS by ethnic group per 1,000 in the general population, January 2019 – July 2023.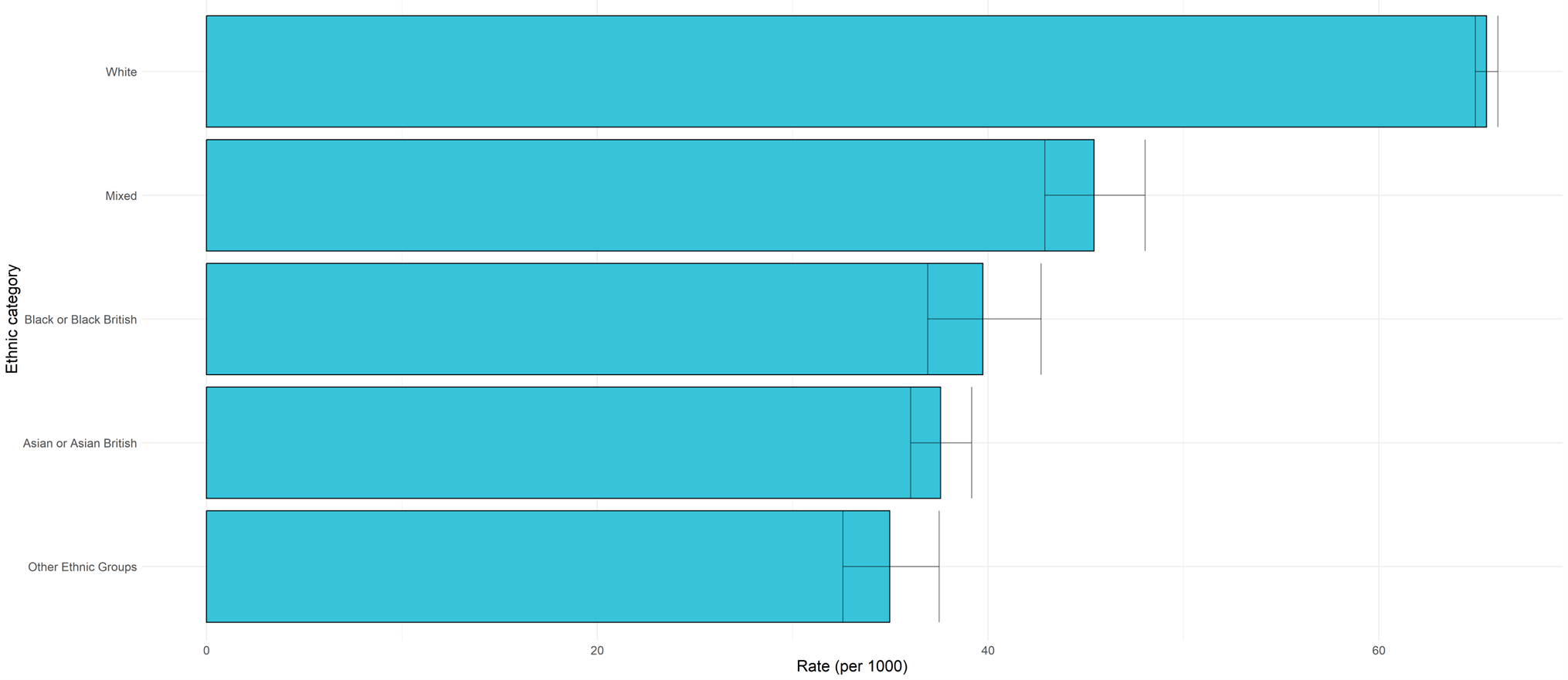
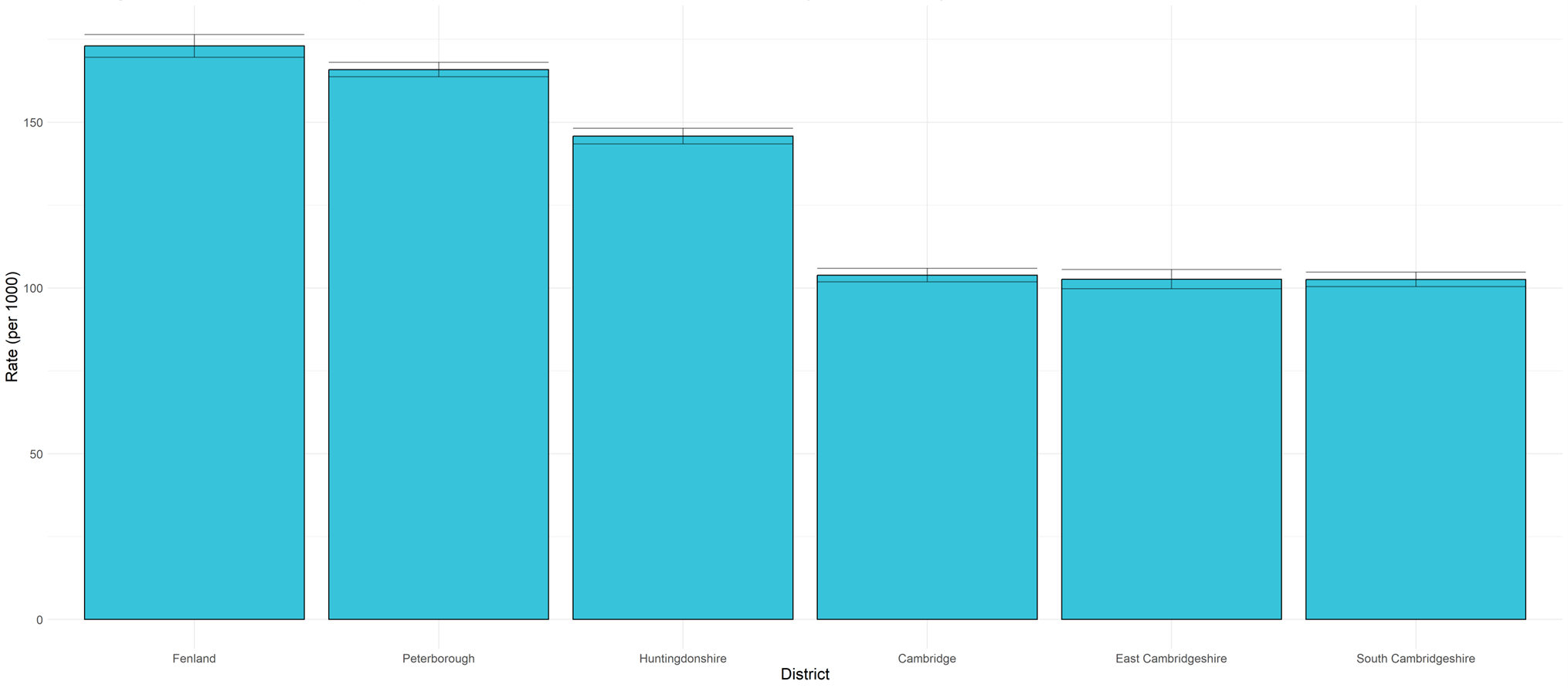
There is a higher rate of referrals accessing the PCMHS from Fenland and Peterborough, compared to other districts. Huntingdonshire also has a high level of referrals, when compared to Cambridge City, East Cambridgeshire and South Cambridgeshire.
Figure 5: Rate of unique referrals accessing PCMHS by district, January 2019 – July 2023.
How effective is this service?
An independent evaluation of the PCMHS in 2018 estimated that this service resulted in an annual saving of at least £650,000, due to a reduction in secondary care referrals and re-referrals to PCMHS (Elliot & Allan, 2018). The evaluation found that (Elliot & Allan, 2018):
- There were strong levels of support for the introduction of this service amongst practitioners and patients.
- Practitioners had positive experiences of working within the PCMHS team. They reported that the ‘buy-in’ to this service from GPs was mixed, although this is improving as the service becomes better established.
- Patients were very positive about their experiences of and outcomes from the service, and particularly appreciated being able to access appointments at their GP surgery.
- Initial feedback from practitioners, patients and GPs suggested that this service is helping to support patient wellbeing and the management of mental health conditions.
Since this evaluation there have been additional developments to the PCMHS team to improve the working partnership with primary care initially as part of the Peterborough Exemplar and in the roll out of the county-wide Stepped Care model.
Community Connector Mental Health Service
Mental Health Community Connectors (MHCCs) were introduced to work with patients with mental health needs, who do not currently need support from specialist community mental health services (Tiffin, 2023). They provide a specialist social prescribing service focussing on mental health need.
- Each community connector works with around 150 individuals per year who:
- are not suitable for Talking Therapies and do not reach thresholds for secondary mental health services.
- currently rely on regular GP appointments for sustained wellbeing, and for whom isolation is a key issue, or their mental health issues are exacerbated by other social issues (such as housing, relationship, physical health, finance/benefits, drugs and alcohol).
- They provide mental health support within primary care, often within the community rather than the practices themselves, and offer longer appointments than GPs. They have a flexible role that aims to meet the needs of individual primary care networks (PCNs) (Tiffin, 2023), including:
- Flexible strengths-based and goal-oriented support within a familiar setting of patient’s general practice.
- Support with accessing and navigating with mental health services, community support and preventative physical health services.
- Coaching and encouragement based on the ‘Five Ways to Wellbeing’.
- A dedicated in-house mental health resource for GPs with expert knowledge and access to further services to ensure patients are navigated to the right place at the right time.
- This role was added to PCNs as part of the NHS England Additional Roles Reimbursement Scheme in 2021, to enable PCNs and mental health providers to work together and place professionals with mental health expertise within primary care.
How many people use this service?
PCNs in Cambridgeshire and Peterborough range in size from around 30,000 to 90,000 people (Primary Care Networks – Overview, 2019). In October 2023, there were:
- 7 mental health community connectors in the North (covering 58% of the 12 PCNs).
- 6 mental health community connectors in the South (covering 67% of the 9 PCNs).
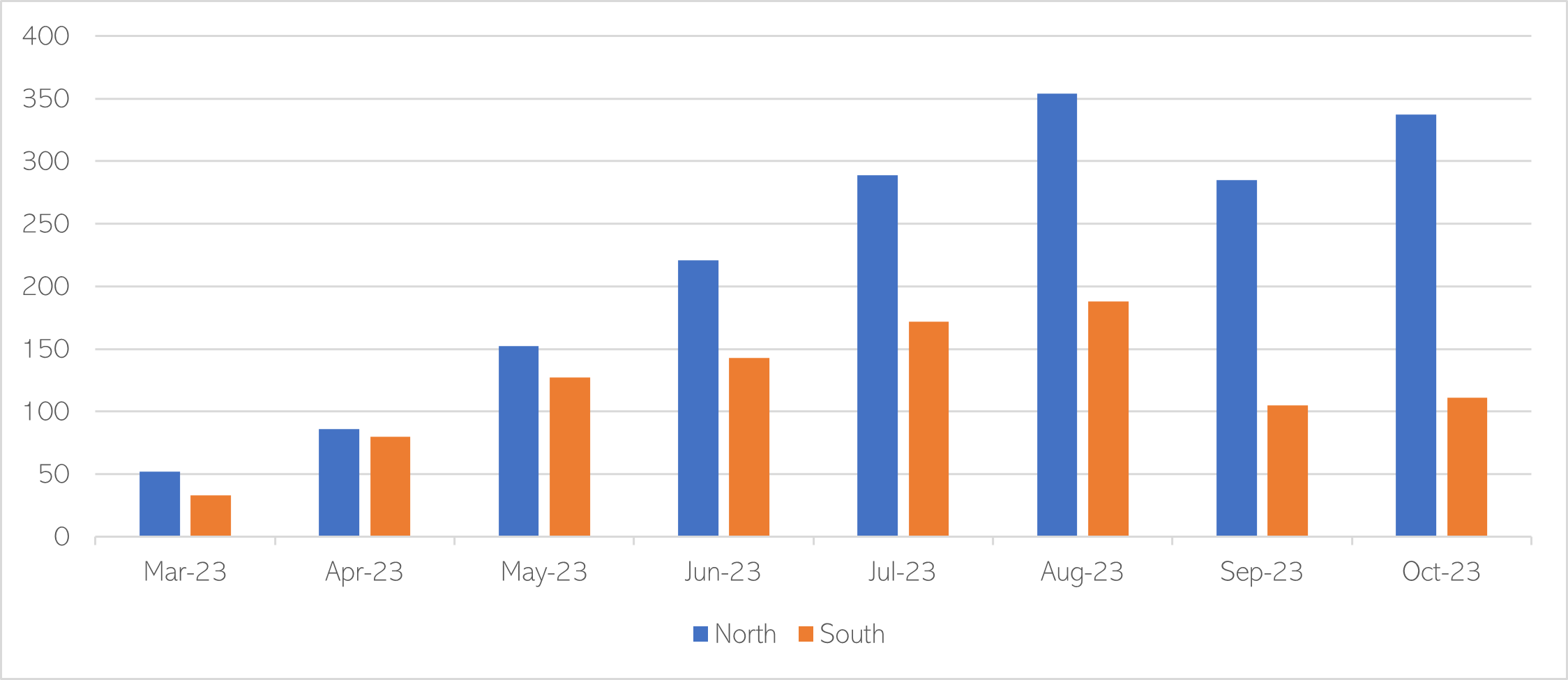
990 people have been referred to Mental Health Community Connectors from February to October 2023, with 281 onward referrals made to relevant mental health organisations. Patients on the service caseload each month for services in the North and South increased steadily from March to August 2023, with a slight decrease after this point.
Figure 6: Active patients on the community connectors caseload each month in North and South, March – October 2023.
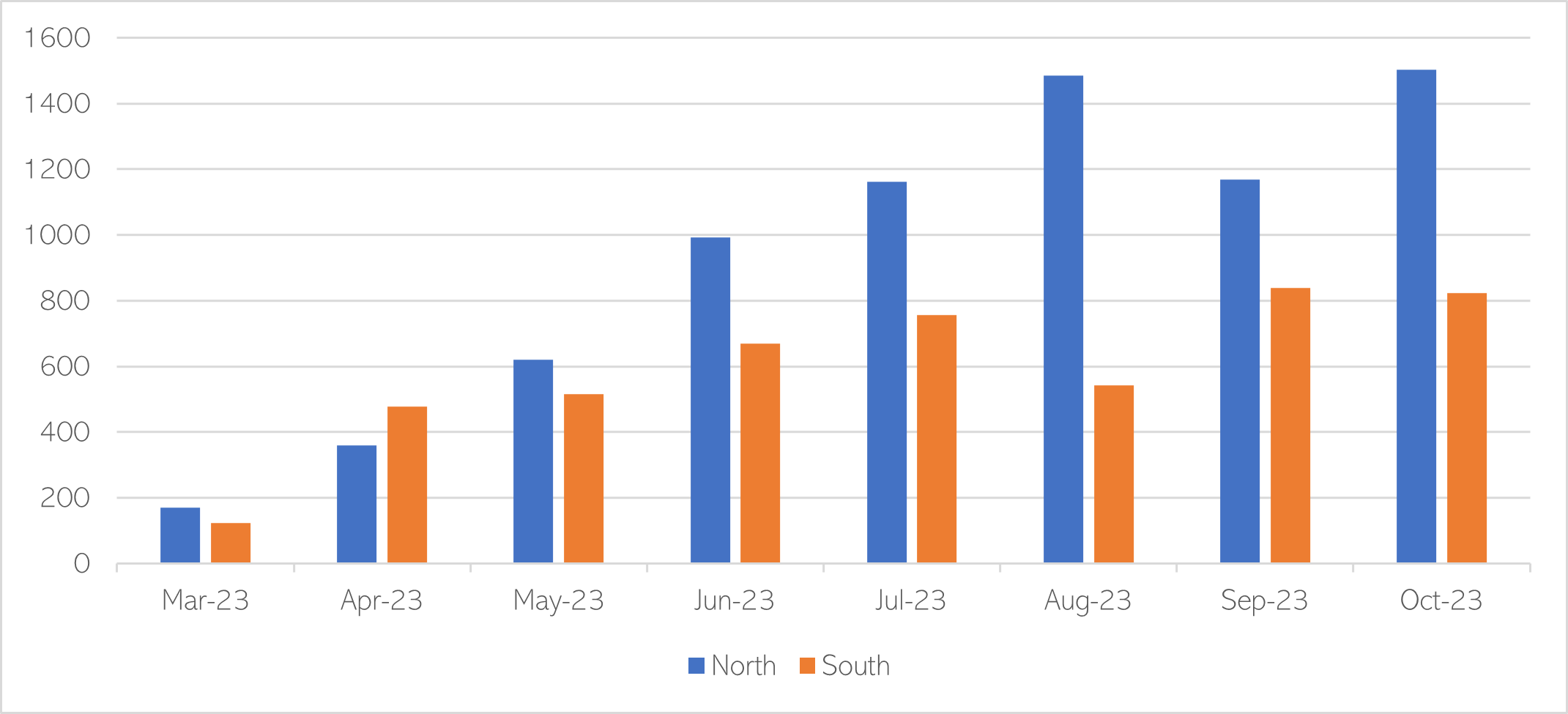
Each patient using this service is likely to receive 7 or 8 activity contacts. The number of patient contacts delivered each month has increased over time, although the average number of patient contacts per month varied somewhat (from 2 to 13) as these services became established. Overall, there have been 12,200 activity contacts across both services from February to October 2023.
Figure 7: Patient contacts from community connectors each month in North and South, March – October 2023.
What do people say about this service?
In October 2023 90% of patients in the North, and 80% in the South, were ‘likely’ or ‘extremely likely’ to recommend the service. Patient satisfaction scores continue to rise each month.
Additional resources
- The local data packs give an overview of prevalence and service use
- Peterborough Exemplar
- Improving access for all: reducing inequalities in access to general practice services
- Data packs for primary care networks in Cambridgeshire and Peterborough, produced in November 2019
- Mental health and primary care networks: Understanding the opportunities
References
Full list of references is included at the end of this chapter.