This chapter of the Cambridgeshire and Peterborough Mental Health Needs Assessment covers the mental health needs of working age adults. We have defined this group as all adults aged between 17 and 64, regardless of employment status. We have used this definition as it is widely used within the NHS and social care and 17 is the cut off for some children and young people’s mental health services. However, many of the services covered here will also cover older adults (aged 65 and above). We also recognise that people may work outside of this age range, particularly as the state pension age is increasing.
There are seven main sections of this chapter: wider policy context and demographics, mental health need, system enablers, interventions for common mental health conditions, interventions for severe mental illness, practical and social support, integrating physical and mental health, and the evidence base for prevention.
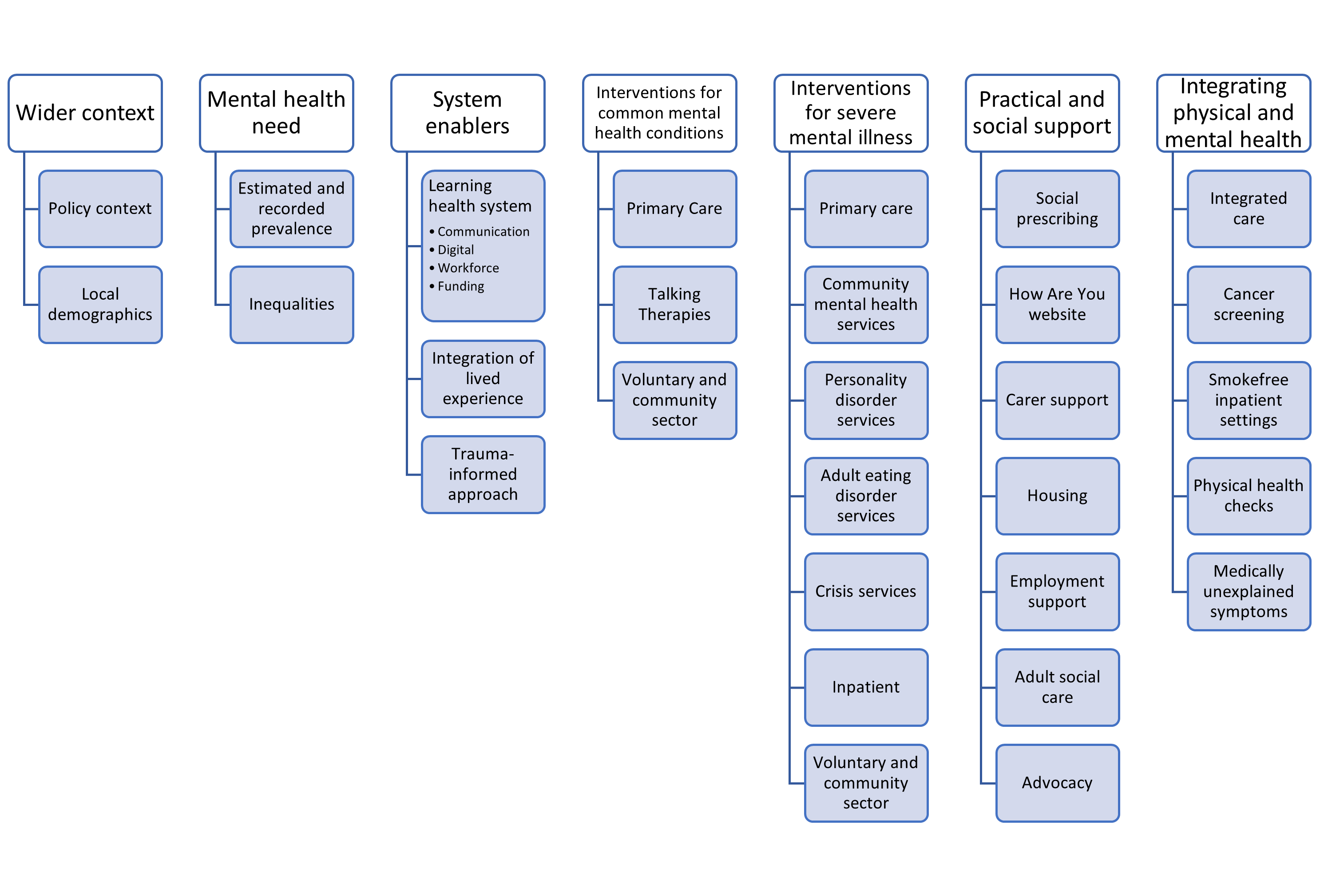
Figure 1: Chapter outline
This chapter can be downloaded as pdfs (part 1 and part 2). You can also view the datapacks to see the estimated prevalence of mental illness and data analysis carried out alongside this chapter.
2025 Updated Prevalence Data
2014 Prevalence Data
The mental health needs assessment is continuously being developed and we encourage people across the system to share insights and links that could be added to this report. This chapter of the mental health needs assessments does not cover the following services:
- Secure mental health services (also known as forensic services). These provide accommodation, treatment and support for people with severe mental illness who pose a risk to themselves and at times, the public (Public Health England, 2019). They predominantly support people who have been imprisoned, or those who have been admitted to hospital through the Mental Health Act following a criminal offence (Durcan, 2011).
- Learning disability services, which are covered in the Health of Adults with a Learning Disability JSNA (2023)
Recommended areas for future work
The following questions were raised in the writing of this chapter and highlight potential future areas of future work needed. These should be read alongside the other areas for future work already highlighted in Chapter Two of this needs assessment, to ensure a focus on the groups of people at highest risk of mental illness and least likely to access services and support at the right time.
Mental health need
- Continue to update and publish estimates of mental health need in Cambridgeshire and Peterborough, in line with national evidence.
- Recognise that demand for services is still affected by COVID-19 and that this needs to underpin short-term service planning.
- Compared the estimated number of people experiencing first-episode psychosis (FEP) in our local population against the number of people who access CAMEO, to assess potential unmet need.
- Develop the system understanding of the prevalence of hoarding in Cambridgeshire and Peterborough and the cost that untreated hoarding disorder on local services.
- Develop system understanding of inequalities in access to mental health services by CORE20PLUS5 subgroups, across the pathway from early intervention to crisis support. Investigate barriers to access.
System enablers
- Recognise and support the development of a learning health system for adults’ mental health.
- Support the work in providers across the system on auditing the use of evidence-based interventions for both common mental health conditions and severe mental illness. Highlight gaps in the provision of effective evidence interventions to the system.
- Outcome measures should be available as part of the development of a learning health system. Support work to record and report on these and highlight inequalities in outcome measures by population groups.
- Where variation in outcomes relates to not using evidence-based practice in line with NICE guidance, highlight and review this at a system level.
- Work towards services routinely being able to answer the following questions:
- Need: Do we understand the needs in the population that is using the service?
- Demand: Who is presenting to services? How has this changed over time? What is the modelling/predictions for the future?
- Supply/Capacity: How well is the system able to meet the needs of the population? What are the key constraints?
- Flow and outcomes: How do people flow through the different services to receive care?
- Inequalities: Which groups of people are less likely to access services/drop out along the way/have poorer experiences and outcomes/do not have their needs met?
- Ensure a continued focus on sharing data across the system to understand the increase in need for support for both common mental health conditions and severe mental illnesses.
- Build the pool of expertise for mental health analysis that is available across the integrated care system. This should involve reviewing and mapping the data analytical expertise currently contributing to understanding of mental health pathways from across different organisations in the ICS.
Funding
- Ensure that the Mental Health Investment Standard is met locally and in line with the needs outlined across the system.
- Develop understanding of system mental health spend by service type, including prevention and early intervention.
- Develop understanding of the cost effectiveness of mental health interventions and the potential to increase allocative efficiency across the mental health system.
Communications
- Establish resources available from across the different parts of the sector (integrated care board, NHS trust, voluntary and community sector, local authorities) that can contribute on system-wide communications strategy.
- Ensure that communication strategies follow an evidence-based approach.
Digital
- Support mental health providers across the system in improving the digital maturity of their organisations.
- Build understanding of how digital health technologies can support the patient journey in terms of:
- Effective treatment or guiding care choices
- Helping people manage their own mental health
- Releasing staff time
Workforce
- Workforce is a major constraint on the system’s ability to meet population needs. Carry out joined-up working to map and model future needs that will contribute to workforce planning across the system.
- Recognise the critical importance of workforce considerations in system decisions.
Integration of lived experience
- Review the systematic inclusion of lived experience alongside other types of data to contribute to developing a learning health system. This should include experience both from people who have used services and those with mental ill health that have not.
- Evaluate mental health services against NICE guidelines for service user experience
Interventions for common mental health conditions
- Evaluate how local services are meeting NICE guidelines around depression in adults and generalised anxiety disorder in adults
- Explore local antidepressant prescriptions, including:
- Prescription rates over time and which diagnoses are linked to antidepressant prescriptions, including insomnia and chronic pain.
- Rates of antidepressant reviews.
- How local services ensure informed consent when initiating and reviewing antidepressants; and if care plans are put in place and shared with patients/carers with clear rationale and expectations around antidepressant reviews and expected duration of treatment.
- Prescribers’ knowledge and confidence around on deprescribing and what support is available for patients who struggle with withdrawal/discontinuation symptoms.
- Exploring the availability and uptake of non-pharmacological interventions for depression and whether they are being fully utilised (in line with NHS England recommendations around optimising personalised care for adults prescribed medicines associated with dependence or withdrawal symptoms)
- Support the development of primary care network and general practice dashboards which include relevant mental and physical health indicators. Work to expand the data available to general practice staff to understand their local population’s use of mental health services, including routine care, crisis care and patient outcomes.
- Investigate re-referral rates in NHS Talking Therapies, including which groups are more likely to be re-referred to this service and the reasons behind this.
Interventions for severe mental illness
- Support the development of learning communities of clinical care between primary and secondary care.
- Explore mental health presentations in ambulance data, across calls and conveyances.
- Analyse who is admitted into inpatient care, segmented by ethnicity, deprivation and diagnosis
- Develop strategy to increase engagement with the Recovery College service.
- Explore antipsychotic prescriptions within Cambridgeshire and Peterborough, in terms of:
- The number of people Peterborough currently on antipsychotic medication but who are not the SMI register, including in terms of demographic factors and diagnoses (learning disability, mental illnesses, dementia and palliative care). Investigate how many people in this group receive annual physical health checks.
- Understand areas needing a focus on deprescribing and how to support this, including for people with a personality disorder diagnosis who are currently on antipsychotics.
- Explore access to depot antipsychotics across Cambridgeshire and Peterborough, to see if there are any geographic inequalities.
- Ensure access to evidence based effective treatments for severe mental illness (for example clozapine, ECT) is equitable, particularly in terms of population groups and geography across the county.
- Investigate the roll out of the Stepped Care model across the county, including the perspectives of people with lived experience, carers and professionals.
Inpatient and Crisis care
- Partners across the crisis system to evaluate and refresh the crisis dashboard, in collaboration with Right Care, Right Place
- Review inpatient bed numbers in line with the Crisp Commission (2016) to model the number of beds needed to ensure average inpatient bed occupancy rates are no more than 85% in line with Royal College guidelines, and to eliminate inappropriate out of area admissions. This review should include local inpatient detox bed provision.
- Use Emergency Department data sources from across the county to understand who presents to this service in mental health crisis.
- Investigate why an increasing proportion of people attending A and E for reasons relating to mental health spend more than 6 or 12 hours in the department, including why this is longer than people attending for their physical health.
- Investigate the increasing length of stay for inpatients using tools from the GIRFT approach
- Develop a plan improve the proportion of those followed up within 72 hours of discharge from hospital.
- Continue the work of the Crisis Concordat to improve pathways and reduce inequalities in people who detained under the Mental Health Act
- Explore SystmOne data on how many people assessed under the Mental Health Act access community support instead of being detained. Explore this by ethnicity and by district.
- Support implementation of the recommendations of the local Mental Health Act Pathway review
- Investigate whether inpatient bed availability is a barrier to people being assessed under the Mental Health Act
- Conduct a review of cases where people return to hospital within 90 days, exploring the contributing system factors.
- Evaluate how local services are meeting NICE guidelines around alcohol-use disorders
- Review options for the provision of a community rehabilitation pathway for people with complex mental health needs.
Practical and social interventions
- Understand the system understanding of how social prescribing services, such as community connectors, may impact demand for mental health services.
- Develop work to increase system understanding of need, demand, supply/capacity, flow and outcomes in social care for mental health.
- Develop work to increase system understanding of future need, demand, supply/capacity, flow and outcomes in supporting housing for people with mental health needs.
- Understand CPFT data on non-statutory social care
- Investigate local barriers to people moving on from supported housing, including the criteria of the housing banding system, wating times and potential facilitators.
- Audit local processes of discharge from inpatient mental healthcare against NICE guidelines and investigate potential housing issues relating to discharge from inpatient mental healthcare. Areas to explore include evaluating if partnership working between agencies promotes optimal discharge, whether people are held back in hospital because they cannot access the right accommodation for them and reviewing the discharge co-ordinator pilot to implement learning.
- Explore if people using carer support services are representative of the local population of people who provide care.
- Investigate the ‘waiting list’ offer for carers.
Integrating physical and mental health
- Understand the mental health needs of people in Cambridgeshire and Peterborough living with long-term physical health conditions.
- Develop understanding around the impact of annual physical health checks on health outcomes. Investigate drop out along the pathway from check to improvement for each elements of the health check.
- Investigate the integration of physical health check data across the system (including inpatient physical health checks)
- Segment Healthy You access and outcomes data for people on the SMI register.
- Investigate eye and dental health needs for people with severe mental illness
- Look at opportunities to better provide physical healthcare through CPFT, including evaluating the GP pilot scheme within CPFT
- Explore extending the Lester tool for use for all people with severe mental illness
- Develop a strategy to improve cancer screening attendance amongst people with severe mental illness