Wider context
- Around 1 in 6 adults in England have a common mental health condition (NHS Digital, 2014). It is estimated that around a third of people with mental health needs access NHS mental health services (Department of Health & Social Care, 2023).
- National Institute for Health and Care Excellence (NCIE) standards and guidelines stress that early recognition and rapid access to biopsychosocial and effective care provides the best outcomes for people with mental illnesses (Public Health England, 2019).
- National evidence shows the commissioning and implementation of mental health services is more variable than for physical health conditions, in terms of funding, the length of period mental health problems often go untreated, and full, rather than partial, access to effective interventions (Public Health England, 2019).
- Mental health services across England are under increasing pressures, including increased demand, the wider impacts of the COVID-19 pandemic (Department of Health & Social Care, 2023) and staff recruitment and retention (Care Quality Commission, 2023).
- The Five Year Forward View for Mental Health (2016) set out recommendations for parity of esteem between physical and mental health across all age groups; tackling inequalities; and for cross-Governmental actions on the wider determinants of health, including housing and social inclusion. This strategy was built on in the NHS Long Term Plan and NHS Mental Health Implementation Plan 2019/20 – 2023/24, which set out new integrated models of community mental health care.
National policy
The key ambitions of the NHS Mental Health Implementation Plan 2019/20 – 2023/24 are summarised below:
- Talking Therapies (previously IAPT):
- Access to Talking Therapies services will be expanded to cover a total of 1.9 million adults and older adults across England.
- All areas will maintain the existing Talking Therapies referral to treatment time and recovery standards (50% recovery rate; 75% of people accessing treatment within 6 weeks; and 95% of people accessing treatment within 18 weeks.)
- All areas will maintain the existing requirement to commission Long Term Conditions Talking Therapies services.
- Severe mental illnesses community care:
- New integrated community models for adults with severe mental illness (including care for people with eating disorders, mental health rehabilitation needs and a ‘personality disorder’ diagnosis) spanning both core community provision.
- Dedicated services will ensure at least 370,000 adults and older adults per year have greater choice and control over their care, and are supported to live well in their communities.
- A total of 390,000 people with severe mental illness will receive a physical health check.
- A total of 55,000 people with severe mental illness a year will have access to Individual Placement and Support (IPS) services.
- The 60% Early Intervention in Psychosis access standard will be maintained and 95% of services will achieve Level 3 NICE concordance.
- Mental health crisis care and liaison: There will be 100% coverage of 24/7 age-appropriate crisis care, via NHS 111, including:
- 24/7 crisis resolution and home treatment functions for adults, operating in line with best practice by 2020/21 and maintaining coverage to 2023/24.
- 24/7 provision for children and young people that combines crisis assessment, brief response and intensive home treatment functions.
- A range of complementary and alternative crisis services to A&E and admission (including in voluntary sector/local authority-provided services) within all local mental health crisis pathways.
- Mental health professionals working in ambulance control rooms, Integrated Urgent Care services, and providing on-the-scene response in line with clinical quality indicators.
- All general hospitals will have mental health liaison services, with 70% meeting the ‘core 24’ standard for adults and older adults.
- Therapeutic acute mental health inpatient care: The therapeutic offer from inpatient mental health services will be improved by increased investment in interventions and activities, resulting in better patient outcomes and experience in hospital. This will contribute to a reduction in length of stay for all services to the current national average of 32 days (or fewer) in adult acute inpatient mental health settings.
Alongside the Long Term Plan, the advancing mental health equalities strategy (2020) had three key focus areas: supporting local health systems to address inequalities in mental health, improving data flow and quality to better inform decision making, and working with partners to promote a representative workforce across all levels of the mental health system.
The Major Conditions Strategy will be released in 2024 and will include a focus on mental illness. This replaces the planned Mental Health and Wellbeing Plan. This national strategy will focus on integrated healthcare, and will have five main focus areas:
- Moving towards a personalised approach to prevention.
- Early diagnosis and treatment in the community.
- The effective management of multiple conditions.
- Closer integration and alignment between physical and mental health services.
- Person-centred services and support, which gives individuals greater choice about their care.
Community mental health framework
The Community Mental Health Framework for Adults and Older Adults sets out the Long Term Plan’s vision to expand and transform community mental health services for adults and older adults with severe mental illnesses. This programme has been co-designed with service users and carers. It sets out that people with mental health conditions will be enabled as active participants rather than passive recipients of disjointed, inconsistent and episodic care. The overall goal of delivering good mental health support, care and treatment in the community is underpinned by the following six aims (NHS England, 2019):
- ‘Promote mental and physical health, and prevent ill health.
- Treat mental health problems effectively through evidence-based psychological and/or pharmacological approaches that maximise benefits and minimise the likelihood of inflicting harm, and use a collaborative approach that: builds on strengths and supports choice; and is underpinned by a single care plan accessible to all involved in the person’s care.
- Improve quality of life, including supporting individuals to contribute to and participate in their communities as fully as possible, connect with meaningful activities, and create or fulfil hopes and aspirations in line with their individual wishes.
- Maximise continuity of care and ensure no “cliff-edge” of lost care and support by moving away from a system based on referrals, arbitrary thresholds, unsupported transitions and discharge to little or no support. Instead, move towards a flexible system that proactively responds to ongoing care needs.
- Work collaboratively across statutory and non-statutory commissioners and providers within a local health and care system to address health inequalities and social determinants of mental ill health.
- Build a model of care based on inclusivity, particularly for people with coexisting needs, with the highest levels of complexity and who experience marginalisation’.
The Community Mental Health Framework replaces the Care Programme Approach (CPA) for community mental health services. It aims to move away from ‘an inequitable, rigid and arbitrary CPA classification’ and replace this with a universal standard of community mental healthcare (NHS England, n.d.).
The COVID-19 Mental Health and Wellbeing Recovery Action Plan (2021) set out additional investment to speed up the roll out of the Community Mental Health Framework.
Personalised care
Personalised care means that ‘patients have more control and choice when it comes to the way their care is planned and delivered, taking into account individual needs, preferences and circumstances’ (PCI, 2024).
The NHS Long Term Plan (2019) set out steps to make personalised care ‘business as usual’, through the roll out of the NHS comprehensive model for personalised care; ensuring 200,000 people benefit from a personal health budget (by 2023/34); and the introduction of new social prescribing link workers, to connect people to resources in their local community, to improve health and wellbeing (NHS, 2024).
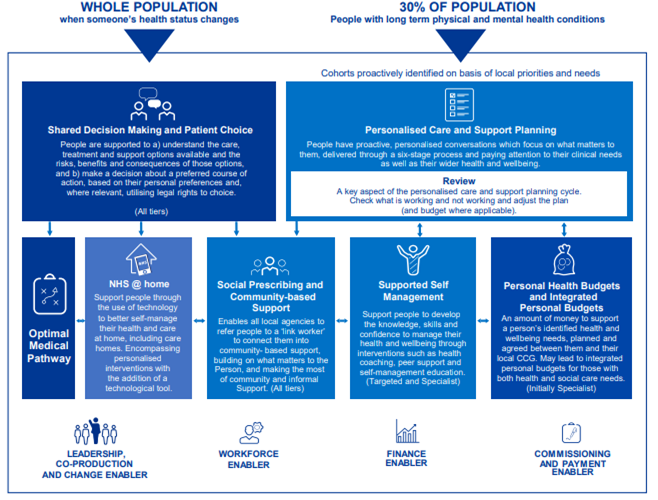
The comprehensive model of personalised care is a framework that sets out 6 evidence-based components of personalised care, to establish a whole-population approach to supporting people to manage their physical and mental health and wellbeing, build community resilience and make informed choices when their health changes (NHS England, 2024).
Figure 1: Personalised care operating model. Image source: NHS England
Local policy
The main local strategy relating to the mental health of working-age adults is the Joint Health and Wellbeing Strategy (2022 – 2030), which was created by Cambridgeshire County Council, Peterborough City County and the Cambridgeshire and Peterborough Integrated Care System. This strategy:
- Set out three overarching ambitions: increasing the number of years people spend in good health; reducing inequalities in preventable deaths before age 75; and achieving better outcomes for children.
- Named four system priorities, including ‘promoting early intervention and prevention measures to improve mental health and wellbeing’.
- Set ‘ensuring health checks for 60% of people living with severe mental illness’ as a specific target to reduce health inequalities.
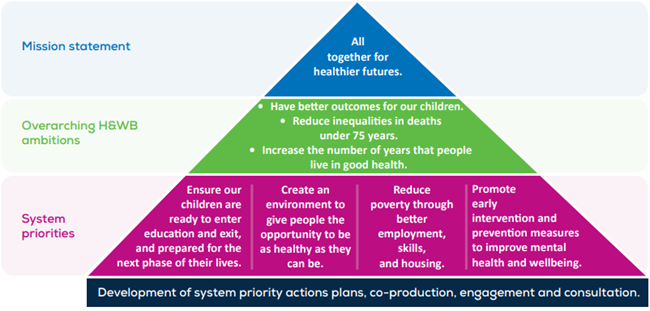
Figure 2: Ambitions of the Joint Health and Wellbeing Strategy. Image source: Joint Health and Wellbeing Integrated Care Strategy
Other relevant strategies include the:
- The Crisis Care Concordat, published in 2014, recognises many of the issues related to the crossover of work by health, social care and emergency services.
- As part of the clinically-led review of NHS access standards, Cambridgeshire and Peterborough received additional funding in 2020/21 to test new models of integrated care and four-week waiting times for community-based mental health services
- All Age Carers Strategy (2018 – 2022)
- Joint Cambridgeshire and Peterborough Suicide Prevention Strategy 2022-2025
- CPFT Strategy (2023 – 2026)
North and South Care Partnerships and Integrated Neighbourhoods
The Cambridgeshire and Peterborough Integrated Care System (ICS) works across the health system, local authorities, voluntary and community sector organisations and the wider community. Within this, there are two ‘Place’ partnerships, covering the North and South of our local areas. Each of these places covers a population of around 575,000 people.
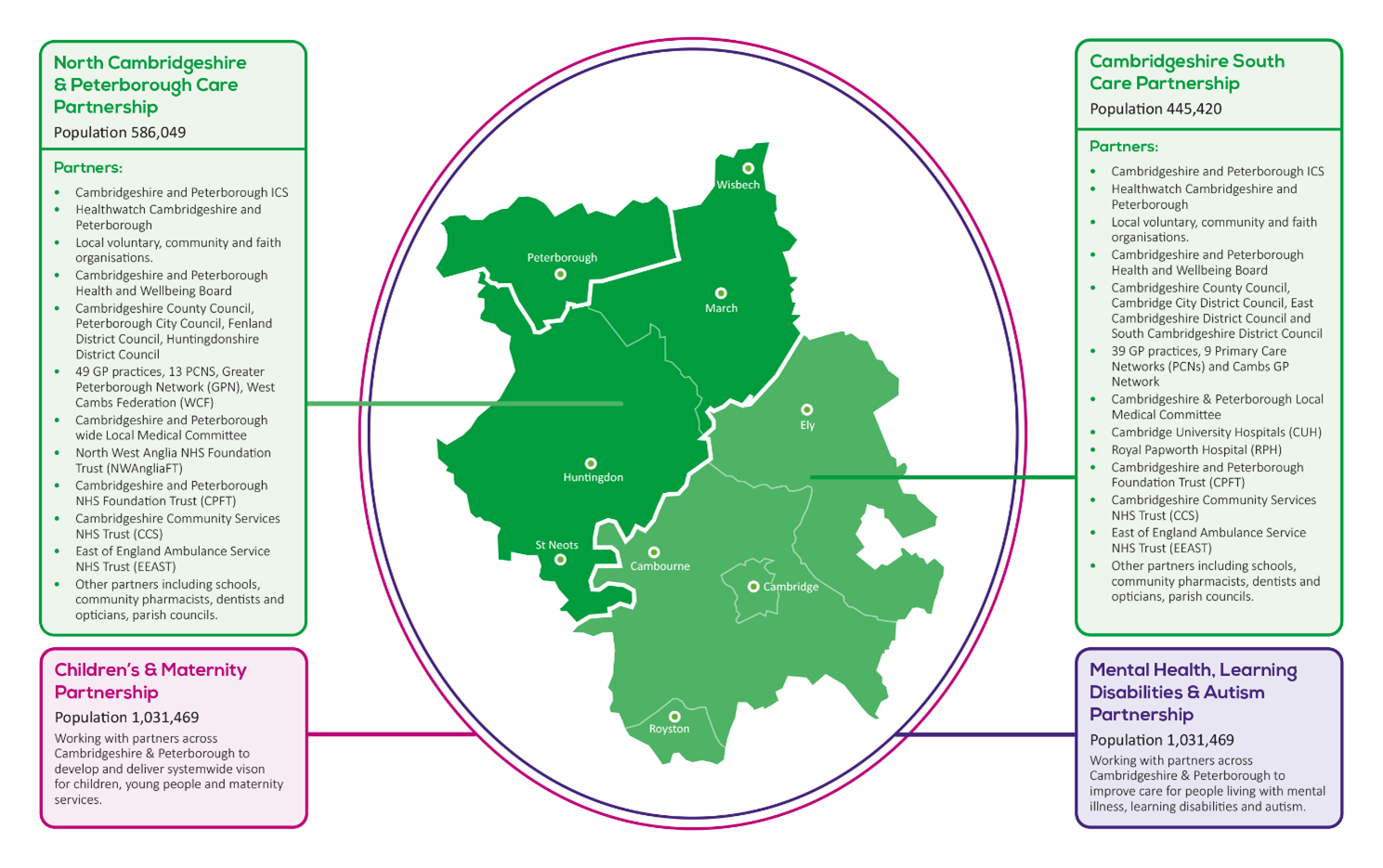
Figure 3: Cambridgeshire and Peterborough Integrated Care System North and South Partnerships
Within the North and South Partnerships, most people’s needs will be delivered through Integrated Neighbourhoods. These are communities of between 30,000 and 50,000 people based around Primary Care Networks (PCNs). The aim for Integrated Neighbourhoods is that ‘local care provision should be proactive, in the right place, and make a difference for the local population, by addressing health inequalities and improving outcomes for our patients’ (Cambridgeshire and Peterborough Integrated Care System, 2023).
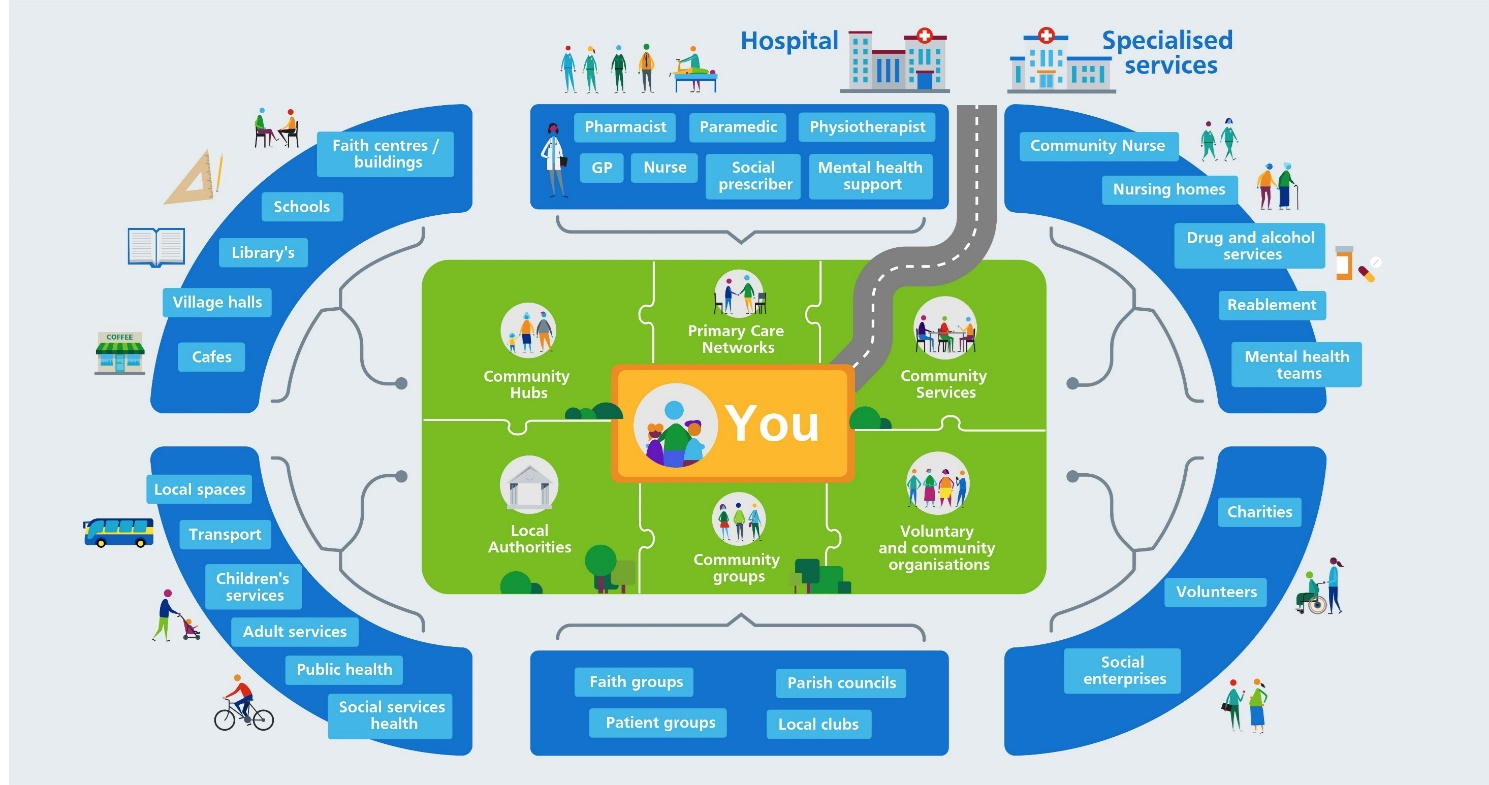
Figure 4: Model of Integrated Neighbourhoods.
Patient and Carer Race Equality Framework
The Patient and Carer Race Equality Framework (PCREF) is one of the key recommendations of the Mental Health Act independent review (NHS England, 2023g). It is community-driven Organisational Competence Framework which should enable trusts to understand what practical steps they need to take to meet the needs of diverse ethnic backgrounds. PCREF is governed by NHS England and is mandatory for NHS trusts from 2023/24.
There are three strands to what PCREF will enable NHS trusts to do:
- Leadership and Governance: ensure that all NHS Mental Health Trusts are fulfilling their statutory duties under core pieces of legislation, such as the Health and Social Care Act 2012 and the Equality Act 2010.
- National Organisational Competencies: guidance on the competencies trusts should develop and ideas on how to do so, in line with local priorities.
- The Patient and Carers Feedback Mechanism: ensure that the patient and carer voice is at the heart of the planning, implementation and learning cycle.
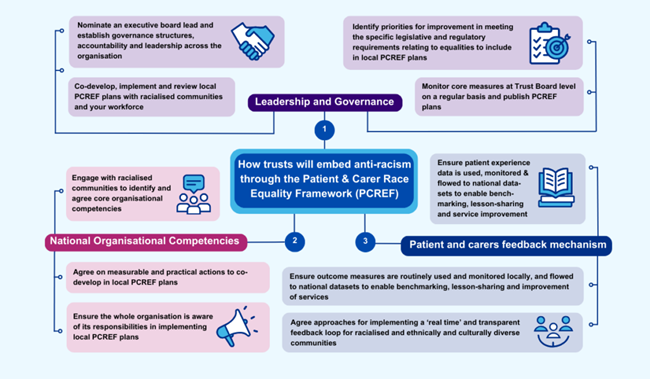
Figure 5: How NHS trusts will embed anti-racism through PCREF. Image source: NHS England
Work to implement PCREF is underway at Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). Current activities include:
- Mapping out what work is already taking place within CPFT that aligns to PCREF guidance.
- Engaging with teams across CPFT about PCREF.
- Work towards a ‘recommendations’ paper for developing a local PCREF plan.
- Starting to review the quality of patient ethnicity data.
Stepped model of care
- The community mental health transformation project of 2019 – 2022 led to a shift from mental health care being provided either within primary care or secondary care, to a stepped model of care.
- With the person firmly at the centre of the model, stepped care is then wrapped around them in increasing levels of intensity and joined together by senior liaison practitioners working across different levels of care, where the most effective yet least resource intensive form of support is provided initially (Public Health England, 2019).
- In Cambridgeshire and Peterborough, this is a place-based stepped care model:
- Community mental health services are wrapped around Primary Care Networks (PCNs) and Integrated Neighbourhoods, so individuals are initially supported by their GP in combination with community-based support, and then in collaboration with the Primary Care Mental Health Service (PCMHS) where further assessment is deemed necessary by their GP.
- Newly formed Neighbourhood Mental Health Hubs bring together practitioners across the system to connect secondary care clinical expertise to the wealth of community assets. Roles such as social prescribing link workers combine these offers.
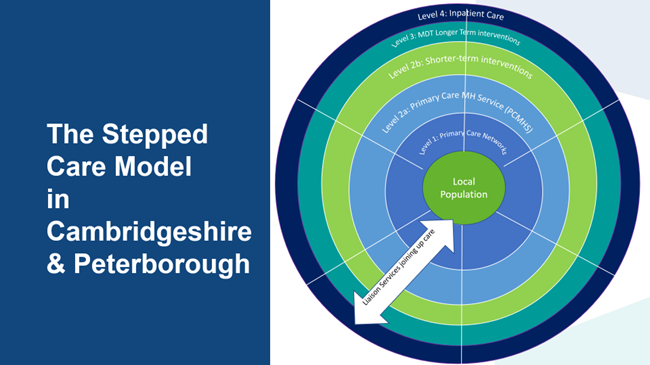
Figure 6: Model of stepped care for in Cambridgeshire and Peterborough.
Additional resources
- The local data packs give an overview of prevalence and service use
- Mental Health Policy in England
- The Community Mental Health Framework for Adults and Older Adults
- Progress in improving mental health services in England
- The Health and Social Care Committee’s Expert Panel: Evaluation of the Government’s progress against its policy commitments in the area of mental health services in England
- For further information about PCREF: NHS England » Advancing mental health equalities and Patient and carer race equality framework: making decisions with communities, not for them
- Personalised Care Institute sets the standards for evidence-based training in personalised care in England
- NHS personalised care operating model
- What is personalised care and support planning?
References
Full list of references is included at the end of this chapter.