Barriers and inequalities
Anyone can be impacted by perinatal mental health conditions, but some groups are more at risk and may face specific barriers to accessing care. This subsection will detail barriers to accessing perinatal mental health support and the local populations who face inequalities in perinatal mental health.
Barriers to accessing support
- Only a small proportion of people with perinatal mental health conditions currently access mental healthcare, with one national review estimating just 9% of women with antenatal depression and 6% with postnatal depression receive adequate treatment (29).
- A large national survey carried out in 2019 of people who had experienced, or their partner had experienced, a mental health problem during the perinatal period found that nearly half (47%) felt it was ‘difficult’ or ‘very difficult’ to access mental health support (30).
Anyone experiencing difficulties with their mental health can face barriers to accessing support (as highlighted in chapter two), but there are also additional barriers specific to the perinatal period. These include:
Structural
- Practical barriers, such as a lack of childcare or inability to take time of work (31).
- Lack of collaborative and integrated care, which can make it difficult to disclose mental health conditions (32).
- Fathers can feel felt reluctant or unable to express their needs for mental health support (33). They may feel that they need to prioritise their partner’s needs, particularly if they perceive that services were under-resourced (33).
Healthcare
- Perceived focus on infant health and wellbeing to the exclusion of parents’ needs (34).
- Professionals lacking understanding of the significance of parental mental health to child development (35), or lacking the time to address psychological needs (32).
- Professionals lacking skills and/or confidence in treating or making referrals for perinatal mental health conditions (32).
- Limited childcare facilities or integration of babies within therapy sessions, which can prevent people from attending appointments (32).
Individual
- Lack of knowledge around perinatal mental health (such as not knowing what to do when symptoms became worse, normalising symptoms due to pregnancy) (32).
- Stigma, guilt and shame around being diagnosed with a perinatal mental health condition (particularly in relation to not fulfilling social expectations around parenthood) (32).
- Fear that medication will be prescribed whilst pregnant or breastfeeding, and that this will harm their baby (32).
- Stigma and fear around losing custody of their child (35), which can mean that some people wait until crisis point before accessing support (34).
Inequalities
Anyone can experience a mental health condition during the perinatal period. A large national survey of people who had experienced, or their partner had experienced, a mental health problem during the perinatal period reflected this, as people felt that their mental health was impacted by severe sickness during pregnancy, physical illness, difficulties with infant feeding, traumatic birth experiences and having a history of mental health conditions (30).
However, some groups experience inequalities in perinatal mental health. They may be more likely to experience poor mental health during the perinatal period or require additional support to have a healthy pregnancy and birth.
- The 2010 Marmot review states that action tackling health inequalities should be universal but proportionate to the level of disadvantage (proportionate universalism) (43). Hence services must respond to each families’ health needs and social situation; and provide increasing support as health inequalities increase (44).
- NICE guidelines identifies that some people with ‘complex social factors’ may face additional barriers to accessing maternity services, and that services should be targeted towards these groups, to improve access (36). Women who attend antenatal care late or receive minimal levels of antenatal care are at higher risk of maternal death (37); and often face barriers to accessing perinatal mental health support.
- The recently developed CORE20PLUS framework highlights maternity care as a key clinical area of focus and prioritises ‘ensuring continuity of care for women from Black, Asian and minority ethnic communities and from the most deprived groups’ (45). This was chosen to address the significant disparities in maternal mortality between different ethnic groups and areas of greater deprivation (46).
- Work to tackle inequalities locally is being led by the Cambridgeshire and Peterborough Better Births Equality and Equity Plan.
 The following factors were identified from risk factors for antenatal and postnatal depression (the most well-researched perinatal mental health conditions) (40). This list of factors was added to through discussions with an expert advisory group of local stakeholders.
The following factors were identified from risk factors for antenatal and postnatal depression (the most well-researched perinatal mental health conditions) (40). This list of factors was added to through discussions with an expert advisory group of local stakeholders.
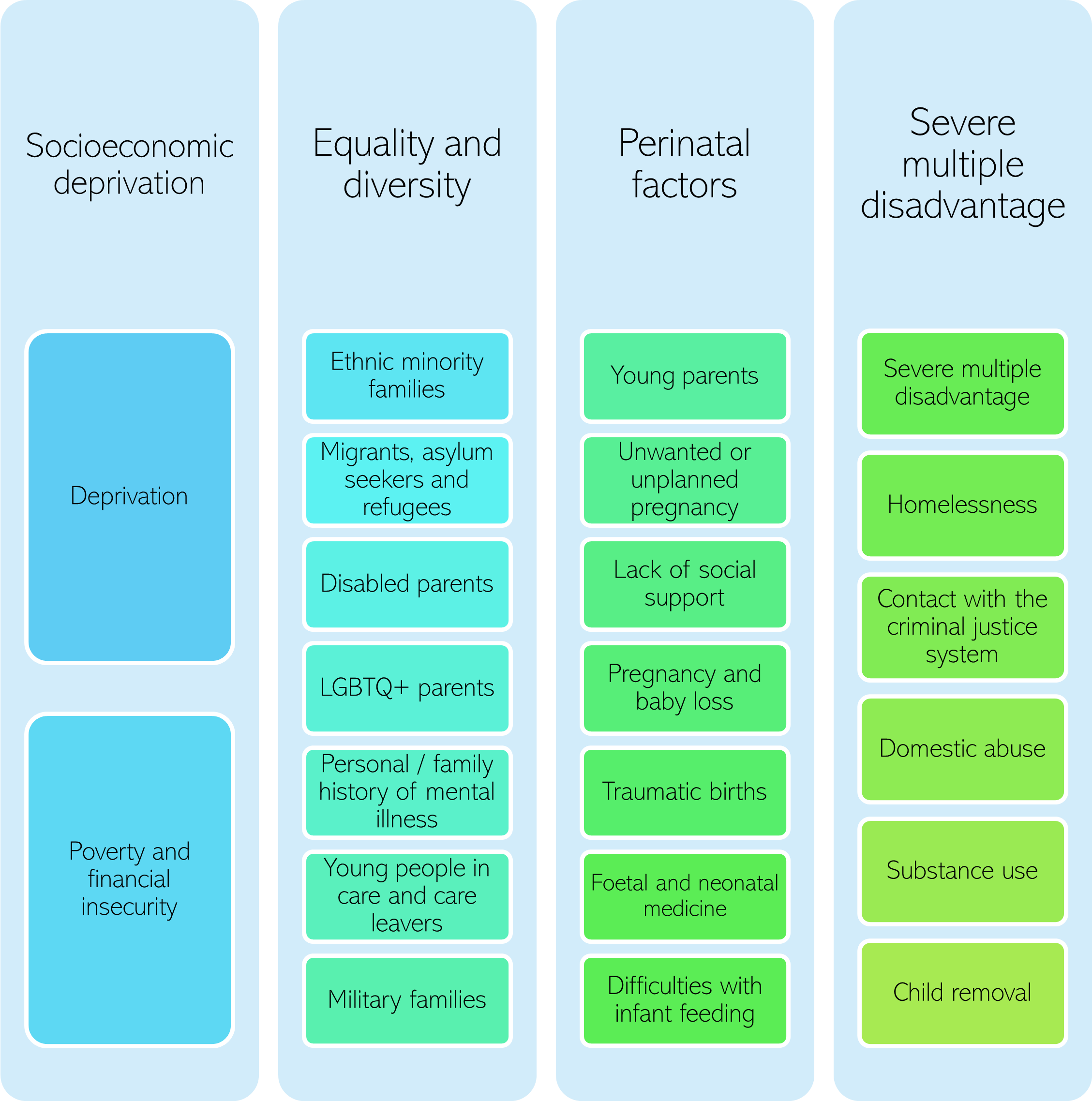
Figure 6: Factors associated with a higher risk of perinatal mental health conditions.
Who is at the greatest risk of perinatal mental health conditions?
The strongest risk factors for antenatal and postnatal depression identified in the literature are:
- Antenatal depression
-
- Strong: domestic violence; prior history of mental health conditions.
- Medium to strong: life stress; anxiety during pregnancy.
- Medium: lack of social support; intention to get pregnant.
- Small: young age.
- Postnatal depression
-
- Strong: domestic violence; previous experiences of abuse.
- Medium to strong: negative life events; lack of social support; migration status; depression, unhappiness or anxiety in pregnancy; history of depression.
- Medium: lack of support from partner; substance use; neuroticism; multiple births; chronic illness.
- Small: low socioeconomic status; family history of any mental health condition; preterm birth.
- Risk factors for postnatal post-traumatic stress disorder (PTSD) include previous traumatic experiences, caesarean section or instrumental birth, prior mental health difficulties and complex pregnancies (41).
- The strongest risk factors for post-partum psychosis are a history of bipolar disorder or previous episodes of psychosis (42). Other risk factors include primiparity (first pregnancy), changes in medication and genetic factors; whilst having a supportive partner is a protective factor (42).
- 1 in 5 women with bipolar disorder suffer a severe recurrence after delivery; and half experience some form of mood disorder in the postnatal period (including major depression) (42).
- A substantial proportion of women with pre-pregnancy eating disorders experience continued or recurring symptoms post-partum (40). Pregnancy is also a high-risk period for the onset of binge eating disorder (43).
- Some risk factors have been under-researched in the perinatal mental health field: for example, few UK studies have investigated the separate impacts of migration and ethnicity on perinatal mental health (44). It is also important to note that many of these factors interact: for example, there are strong association between deprivation and ethnicity, and infant mortality rates (45).
- Furthermore, whilst the focus on this needs assessment is on the services that provide individual-level prevention and intervention of perinatal mental health conditions, it is important to note that social determinants of health (including housing, poverty, racism, and gender-based violence) are the strongest upstream risk factors for poor mental health during the perinatal period (46). Past history of mental illness is an equally important risk factor, which highlights the importance of preconception health (2,47).
Additional resources
- The local data pack gives an overview of key data and trends
- Tackling inequality in maternal health: Beyond the postpartum
- Five steps to reduce inequalities in healthcare
- Equity and equality: Guidance for local maternity systems
- Peterborough & Hinchingbrooke Maternity Voices Partnership and Rosie Maternity and Neonatal Voices Annual Report 2022
- Maternal Mental Health: Women’s Voices
- The Raham Project helping ethnic minority families
References
2. Howard LM, Khalifeh H. Perinatal mental health: a review of progress and challenges. Vol. 19, World Psychiatry. 2020.
29. Byatt N, Xiao RS, Dinh KH, Waring ME. Mental health care use in relation to depressive symptoms among pregnant women in the USA. Arch Womens Ment Health. 2016;19(1).
30. Healthwatch. Mental Health and The Journey to Parenthood [Internet]. 2019 [cited 2023 Mar 1]. Available from: https://www.healthwatchcambridgeshire.co.uk/sites/healthwatchcambridgeshire.co.uk/files/20190904%20Mental%20Health%20and%20Maternity%20Report%20%20FINAL%20%20-%20Compressed%20Webready_0_0.pdf
31. Vigod SN, Dennis CL. Advances in virtual care for perinatal mental disorders. Vol. 19, World Psychiatry. 2020.
32. Smith MS, Lawrence V, Sadler E, Easter A. Barriers to accessing mental health services for women with perinatal mental illness: Systematic review and meta-synthesis of qualitative studies in the UK. Vol. 9, BMJ Open. 2019.
33. Darwin Z, Domoney J, Iles J, Bristow F, Mcleish J, Sethna V. Involving and supporting partners and other family members in specialist perinatal mental health services: Good practice guide [Internet]. 2021 [cited 2023 Feb 16]. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/03/Good-practice-guide-March-2021.pdf
34. Megnin-Viggars O, Symington I, Howard LM, Pilling S. Experience of care for mental health problems in the antenatal or postnatal period for women in the UK: a systematic review and meta-synthesis of qualitative research. Vol. 18, Archives of Women’s Mental Health. 2015.
35. Department of Health. Perinatal Positive Practice Guide [Internet]. 2009 [cited 2023 Feb 6]. Available from: https://www.bl.uk/collection-items/perinatal-positive-practice-guide
36. National Institute for Health and Care Excellence. Pregnancy and complex social factors: a model for service provision for pregnant women with complex social factors [Internet]. 2010 [cited 2023 Mar 24]. Available from: https://www.nice.org.uk/guidance/cg110
37. Nair M, Kurinczuk JJ, Brocklehurst P, Sellers S, Lewis G, Knight M. Factors associated with maternal death from direct pregnancy complications: A UK national case-control study. BJOG. 2015;122(5).
38. NHS England, NHS Improvement. NHS pledges to improve equity for mothers and babies and race equality for staff [Internet]. 2021 [cited 2023 Feb 17]. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/09/C0734-ii-pledges-to-improve-equity-for-mothers-and-babies-race-equality-for-all-staff.pdf
39. NHS England, NHS Improvement. Equity and equality: Guidance for local maternity systems [Internet]. 2021 [cited 2023 Mar 1]. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/09/C0734-equity-and-equality-guidance-for-local-maternity-systems.pdf
40. Howard LM, Molyneaux E, Dennis CL, Rochat T, Stein A, Milgrom J. Non-psychotic mental disorders in the perinatal period. Vol. 384, The Lancet. 2014.
41. Simpson M, Schmied V, Dickson C, Dahlen HG. Postnatal post-traumatic stress: An integrative review. Vol. 31, Women and Birth. 2018.
42. Jones I, Chandra PS, Dazzan P, Howard LM. Bipolar disorder, affective psychosis, and schizophrenia in pregnancy and the post-partum period. Vol. 384, The Lancet. 2014.
43. Watson H, Harrop D, Walton E, Young A, Soltani H. A systematic review of ethnic minority women’s experiences of perinatal mental health conditions and services in Europe. PLoS One. 2019;14(1).
44. Moore L, Jayaweera H, Redshaw M, Quigley M. Migration, ethnicity and mental health: evidence from mothers participating in the Millennium Cohort Study. Public Health. 2019;171.
45. Draper ES, Gallimore ID, Smith LK, Matthews RJ, Fenton AC, Kurinczuk JJ, et al. Maternal, Newborn and Infant Clinical Outcome Review Programme MBRRACE-UK Perinatal Mortality Surveillance Report [Internet]. 2022 [cited 2023 Jan 31]. Available from: https://www.npeu.ox.ac.uk/assets/downloads/mbrrace-uk/reports/perinatal-surveillance-report-2020/MBRRACE-UK_Perinatal_Surveillance_Report_2020.pdf
46. Ormel J, Cuijpers P, Jorm AF, Schoevers R. Prevention of depression will only succeed when it is structurally embedded and targets big determinants. Vol. 18, World Psychiatry. 2019.
47. Public Health England. Making the Case for Preconception Care: Planning and preparation for pregnancy to improve maternal and child health outcomes [Internet]. 2018 [cited 2023 Mar 2]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/729018/Making_the_case_for_preconception_care.pdf