Local picture
Perinatal mental health conditions can be defined as those that occur during the perinatal period (defined here as the period from pregnancy to 2 years after birth) (1). It includes conditions that arise during this time, and those that were present before pregnancy. Up to 1 in 4 women and birthing people will experience perinatal mental illness, making this of the most common type of health condition during this period (1,17).
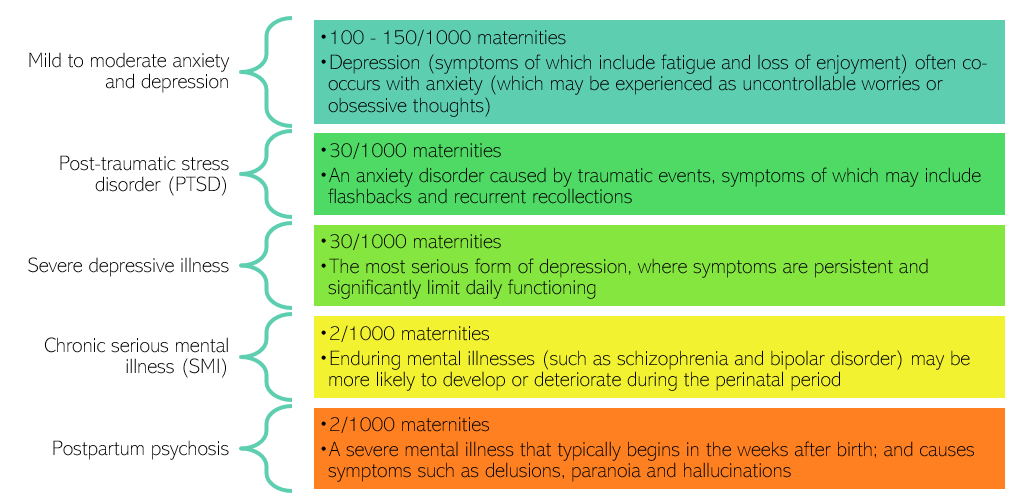
Figure 3: Estimated numbers of people impacted by perinatal mental illness. Adapted from: (18). Note that some people may experience multiple conditions.
- Women and birthing people are around 22 times more likely to be admitted as an inpatient to a mental health unit in the month following birth, compared to pre-pregnancy (19).
- Many cases of perinatal mental illness go unrecognised: around 70% of women with perinatal mental health problems hide or downplay their illness (18); and only half the cases of perinatal depression and anxiety are detected (20).
Estimated prevalence
Using the data above, estimates have been made for the local prevalence of mental health conditions during the perinatal period each year.
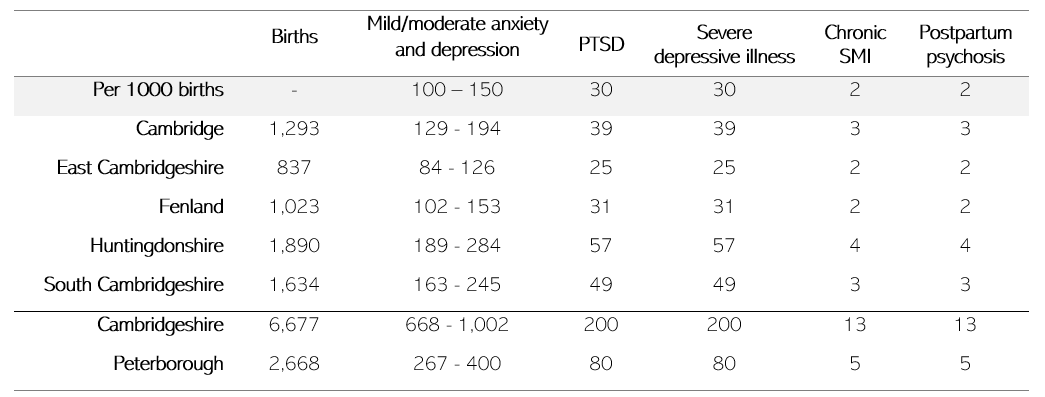
Table 6: Estimated number of cases of perinatal mental health conditions across Cambridgeshire and Peterborough, based on prevalence rates and births in 2021. Data sources: (16,21). Note that some people will have multiple perinatal mental health conditions, so the total number of people impacted will not equal the sum across all conditions.
A group of local stakeholders who formed the expert advisory group for this chapter stated that these numbers are an underestimate of local need, based on their experience in frontline services. Findings of the Perinatal Mental Health survey for Rosie Maternity and Neonatal Voices support this (118):
- The majority (68%) of respondents reported having some kind of mental health concern but only 7% of respondents had a mental health diagnosis.
- 14% of respondents stated that they had developed mental health issues for the first time during the perinatal period whilst 37% of respondents reported having mental health issues in the past.
Maternal mood reviews
At 6 – 8 weeks and 12 months after birth, health visitors carry out maternal mood reviews during development checks. These checks cover a high proportion of families in Cambridgeshire and Peterborough. For those assessed in the maternal mood review carried out at 6 – 8 weeks post-birth:
- In Peterborough, around 13% were likely to have depression and 2% were likely to have severe anxiety.
- In North Cambridgeshire, between 14 and 15% were likely to have depression, whilst levels of severe anxiety varied between 1 to 2%.
- In South Cambridgeshire, an increasing proportion were identified as being likely to have depression, with over double the rate in Q3 (11%) compared to Q1 (5%).
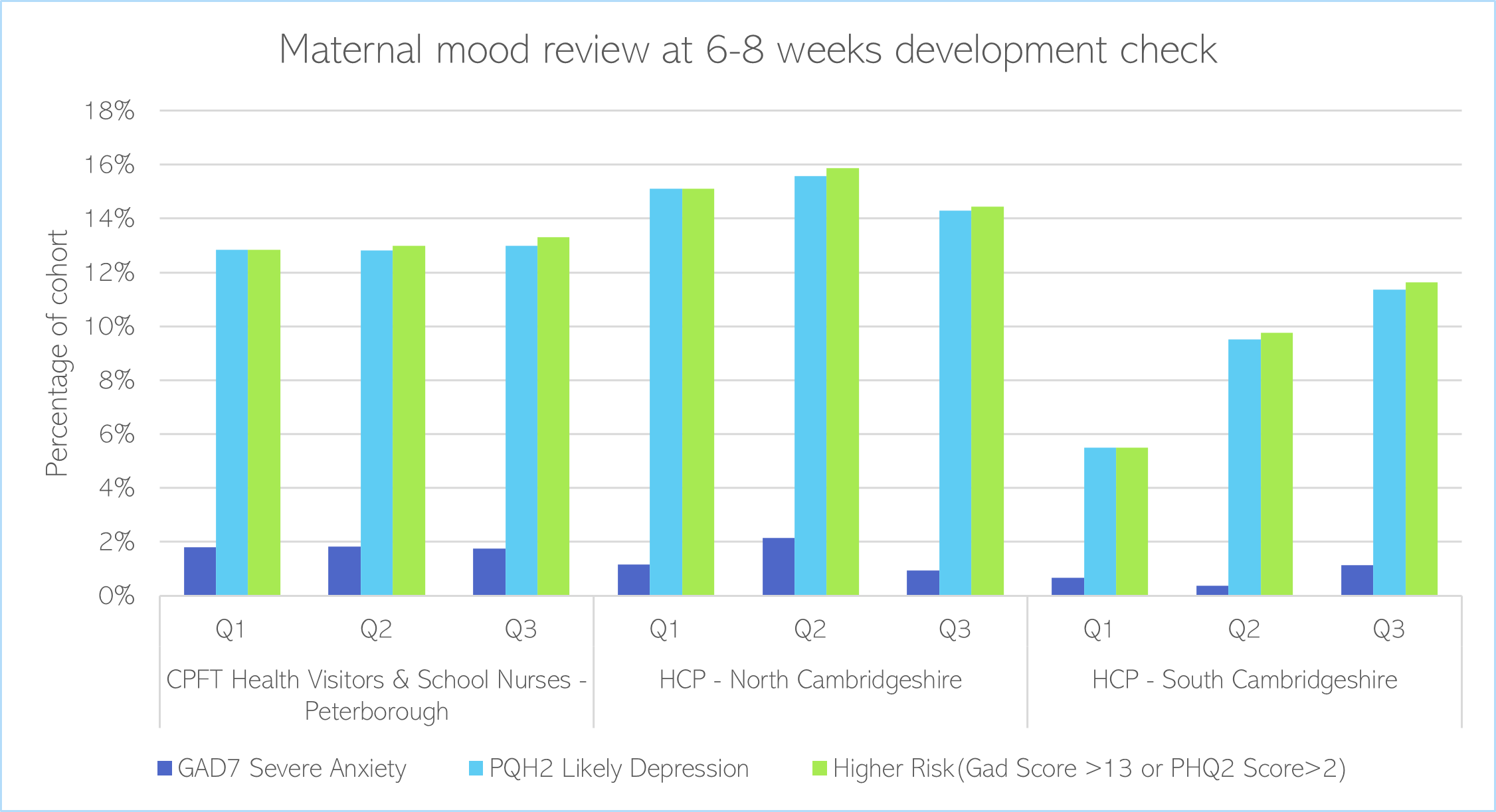
Figure 4: Maternal mood review at 6-8 weeks development check, Q1-Q3 2022/23. Data source: Healthy Child Programme. Note: the Generalised Anxiety Disorder Assessment (GAD-7) is a seven-item instrument that is used to assess the severity of generalised anxiety disorder; whilst PHQ2 is a rapid screening test to identify whether a person may be at risk for depression.
Of the cohort assessed in the maternal mood review carried out 12-months post-birth, the levels of depression remained high in Peterborough, but not in North or South Cambridgeshire:
- In Peterborough, a high proportion were likely to have depression or were at high risk for poor mental health (ranging from 4 to 6%); and there was a sharp increase in people meeting the threshold for severe anxiety in Q3.
- In North Cambridgeshire, around 2% met criteria for likely depression and under 1% for severe anxiety.
- In South Cambridgeshire, a very low proportion were identified as being likely to have depression or severe anxiety.
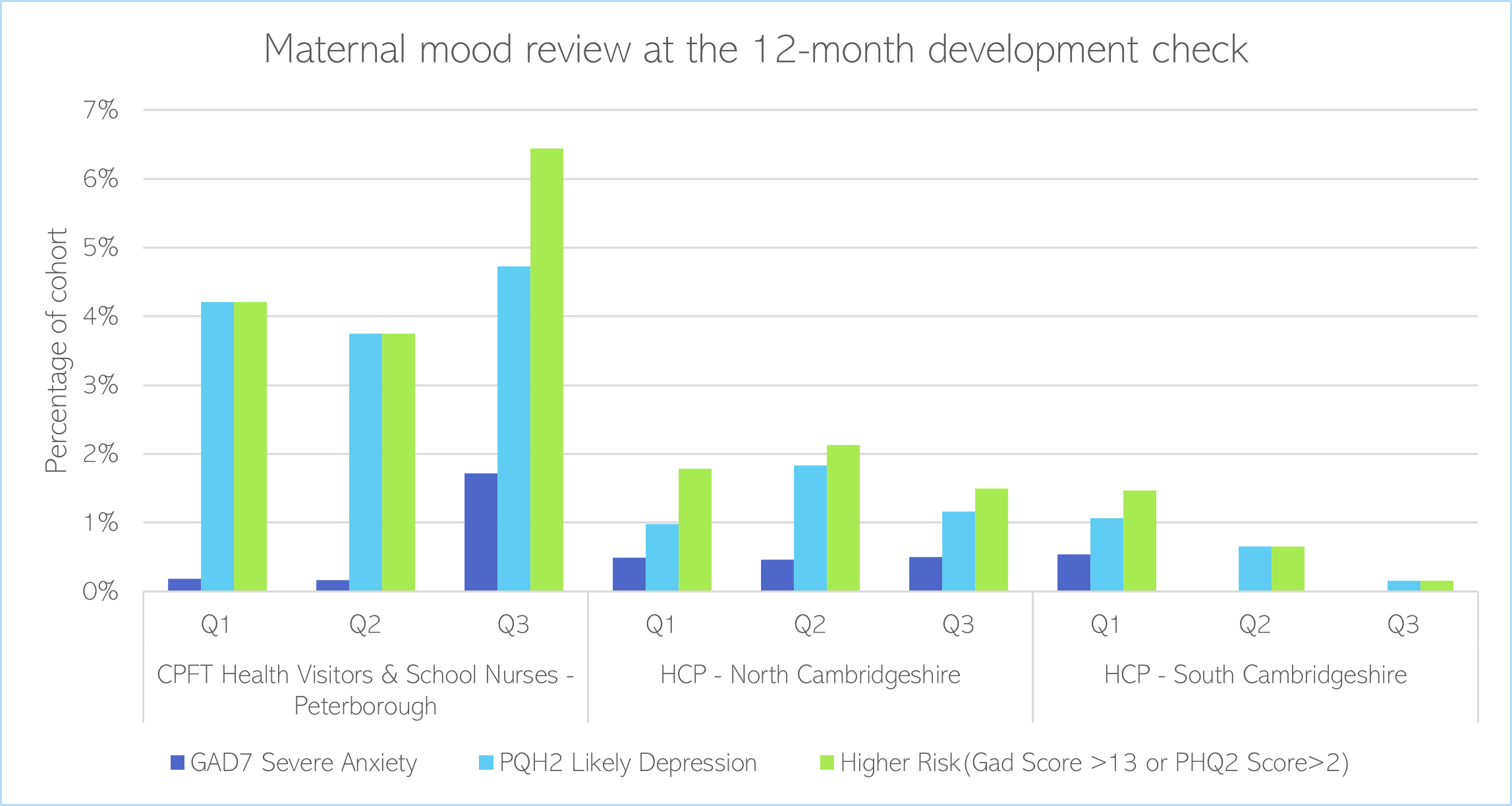
Figure 5: Maternal mood review at 6-8 weeks development check, Q1-Q3 2022/23. Data source: Healthy Child Programme. Note: the Generalised Anxiety Disorder Assessment (GAD-7) is a seven-item instrument that is used to assess the severity of generalised anxiety disorder; whilst PHQ2 is a rapid screening test to identify whether a person may be at risk for depression.
Local population
The fertility rate is higher than the national average in Peterborough, but lower than the national average in Cambridgeshire (15).
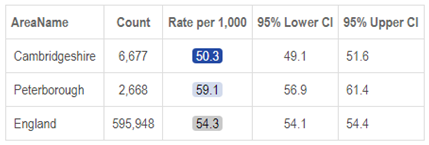
Table 4: Fertility rate per 1,000 of the population in Cambridgeshire and Peterborough in 2021, relative to national rates. Image source: Fingertips. Note: dark blue indicates scores that are lower than the national average; and light blue scores that are higher than the national average.
There were over 9,000 births in Cambridgeshire and Peterborough in 2021.
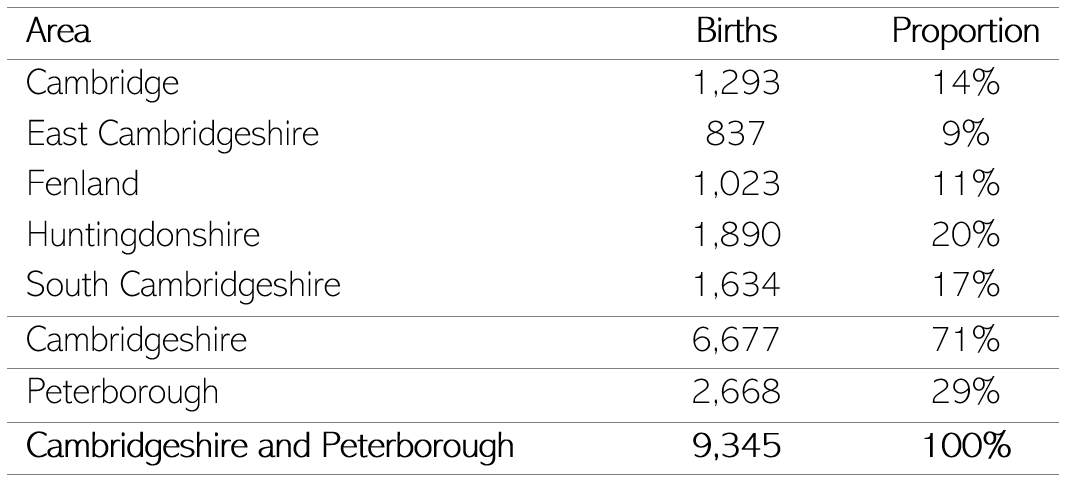
Table 5: Births in Cambridgeshire and Peterborough in 2021. Data source: (16)
Maternal deaths
Maternal deaths are any deaths occurring during the perinatal period. There were 536 maternal deaths nationally between 2018 and 2020 (7). There are substantial inequalities in national maternal mortality rates (7):
- Compared to White women, Black women are 3.7 times more likely, and Asian women are 1.8 times more likely, to die during the perinatal period.
- 1 in 9 women who died during the perinatal period faced severe and multiple disadvantage (SMD).
Suicide is a leading cause of national maternal deaths, accounting for 30% of deaths in 2018-20 (7).
- In 2020, women were 3 times more likely to die by suicide during or up to 6 weeks post-pregnancy (1.5 per 100,000) compared to 2017-19 (0.5 per 100,000). There was a particular increase in the deaths of young women, many of whom were care leavers (note: these figures may have been impacted by the start of the COVID-19 pandemic).
- At least half the women who died by suicide had multiple experiences of adversity, including a history of childhood and/or adult trauma, domestic abuse and having spent time in care.
- Very few women had a diagnosed mental health condition, and many struggled to engage with health and social care services, for a range of reasons including fear of child removal.
Infant mental health
- Infant mental health can be defined as infants’ ability to ‘experience, regulate, and express emotions, form close and secure relationships, and explore the environment’ (22).
- Positive experiences and good relationships with carers form the basis of infants’ mental health (23,24):
- The ability of infants to obtain comfort from their caregiver when distressed (secure attachment) is associated with a range of positive outcomes, including emotional, social and school achievement.
- Insecure and disorganised attachment are associated with an increased risk of mental health conditions later in life. Around 15 – 19% of infants have disorganised attachment, which increases to up to 40% in disadvantage populations and 80% in maltreated populations.
- Chronic stress in early childhood, which can be caused by abuse, neglect or extreme poverty, has a negative impact on babies’ development and can have long-term consequences on their mental health (3).
Co-parent and partner mental health
The perinatal period is a time of huge change for all family members. Fathers and partners have to manage their own mental health, and cope with changing relationships and a new baby. If the birth parent experiences a perinatal mental health condition, this is likely to have an impact on their whole family.
- More than 1 in 3 new fathers report being concerned about their mental health (25). During the perinatal period, around 1 in 10 fathers experiences depression (26); and up to 18% experience anxiety in the postnatal period (27).
- The prevalence of perinatal mental health conditions in step-parents, co-mothers and trans/non-binary parents is unknown. However, some evidence suggests that there are particularly high rates of depression in lesbian co-parents and step-fathers during the perinatal period (28).
- LGBTQ+ parents can face distinct challenges during pregnancy, related to discrimination, marginalisation, and legal recognition as parents (28).
- Mental health between parents is often correlated: for example, between 42 to 50% of partners of mothers receiving inpatient mental health care experience depression (28).
- According to the Perinatal Mental Health survey carried out by Rosie Maternity and Neonatal Voices , 3.4% of survey respondents highlighted that fathers/second parents with mental health issues also need to be supported (118).
Additional resources
-
- The local data pack gives an overview of key data and trends
- NIHR summary of the importance of perinatal factors to public mental health
- MBRRACE-UK: Saving Lives, Improving Mothers’ Care 2022
- Perinatal mental health leaflets written jointly by perinatal psychiatrists, women with lived experience of perinatal mental illness, and their partners.
- Information about complex-PTSD
- Mental health in pregnancy, the postnatal period and babies and toddlers: Report for NHS Cambridgeshire and Peterborough CCG
- Mental Health and Wellbeing: Pre-birth to Age 25 years Needs Assessment
- Parent-Infant Foundation Implementation Toolkit
- Early Years in Mind resources from the Anna Freud Centre
- Recent research highlighting the importance of father’s mental health
References
- Office for Health Improvement and Disparities. Child and Maternal Health [Internet]. Fingertips. 2023 [cited 2023 Mar 20]. Available from: https://fingertips.phe.org.uk/profile/child-health-profiles/data#page/1/gid/1938133228
- Office for National Statistics. Births in England and Wales: summary tables [Internet]. 2023 [cited 2023 Feb 15]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/datasets/birthsummarytables
- Howard LM, Ryan EG, Trevillion K, Anderson F, Bick D, Bye A, et al. Accuracy of the Whooley questions and the Edinburgh Postnatal Depression Scale in identifying depression and other mental disorders in early pregnancy. British Journal of Psychiatry. 2018;212(1).
- Maternal Mental Health Alliance. Perinatal mental health [Internet]. 2023 [cited 2023 Feb 2]. Available from: https://maternalmentalhealthalliance.org/about/perinatal-mental-health/
- Kendell RE, Chalmers JC, Platz C. Epidemiology of puerperal psychoses. British Journal of Psychiatry. 1987;150(MAY.).
- Elliott I. Poverty and mental health: A review to inform the Joseph Rowntree Foundation’s Anti-Poverty Strategy. Mental Health Foundation. 2016;(August).
- Royal College of General Practitioners, Royal College of Psychiatrists. Guidance for commissioners of perinatal mental health services [Internet]. 2018 [cited 2023 Feb 2]. Available from: https://maternalmentalhealthalliance.org/wp-content/uploads/Joint-Commissiong-Panel-perinatal-mental-health-services.pdf
- Simpson TE, Condon E, Price RM, Finch BK, Sadler LS, Ordway MR. Demystifying Infant Mental Health: What the Primary Care Provider Needs to Know. Journal of Pediatric Health Care. 2016;30(1).
- NSPCC. Looking after infant mental health: our case for change – a summary of research evidence [Internet]. 2016 [cited 2023 Mar 8]. Available from: https://library.nspcc.org.uk//HeritageScripts/Hapi.dll/search2?searchTerm0=C6015
- Barlow J, Schrader-Mcmillan A, Axford N, Wrigley Z, Sonthalia S, Wilkinson T, et al. Review: Attachment and attachment-related outcomes in preschool children – a review of recent evidence. Child Adolesc Ment Health. 2016;21(1).
- National Childbirth Trust. Dads in distress: Many new fathers are worried about their mental health [Internet]. 2015 [cited 2023 Mar 1]. Available from: https://www.nct.org.uk/about-us/media/news/dads-distress-many-new-fathers-are-worried-about-their-mental-health
- Paulson JF, Dauber S, Leiferman JA. Individual and combined effects of postpartum depression in mothers and fathers on parenting behavior. Pediatrics. 2006;118(2).
- Leach LS, Poyser C, Cooklin AR, Giallo R. Prevalence and course of anxiety disorders (and symptom levels) in men across the perinatal period: A systematic review. Vol. 190, Journal of Affective Disorders. 2016.
- Darwin Z, Domoney J, Iles J, Bristow F, Siew J, Sethna V. Assessing the Mental Health of Fathers, Other Co-parents, and Partners in the Perinatal Period: Mixed Methods Evidence Synthesis. Vol. 11, Frontiers in Psychiatry. 2021.