Services for all parents and infants
Maternity and health visiting services have frequent contact with parents throughout the perinatal period. This makes them well-placed to identifying people at risk of, or who have, perinatal mental health conditions (10). Professionals in these services also ask about emotional wellbeing at each routine contact, providing support and referring people to specialist services where relevant (110).
Figure 32: Wider support for families and infants during the perinatal period
Maternity services
Families have regular contact with midwives, who provide support throughout pregnancy. Part of midwives’ role includes asking about mental health history and identifying experiencing symptoms of poor mental health (156).
- Midwives work collaboratively with primary and secondary care services and voluntary sector organisations; and refer individuals into mental health support services (156).
- Specialist mental health midwives can (10):
- Provide direct support to people with mental health conditions.
- Be a key point of contact for mental health services, primary care, and social services.
- Provide training and advice for other professionals managing perinatal mental health conditions.
- Receiving midwife-led continuity of care results in a 16% reduced risk of baby loss and 24% reduced risk of pre-term birth (157). Having a trusting relationship with a healthcare professional is important to regaining trust in healthcare systems for women with experiences of trauma, or social risk factors (158).
- Nationally, there is a shortage of midwives (159). National evidence suggests that some midwives do not enquire about their patients’ mental health as they feel pressurised for time and are nervous about uncovering issues that could be difficult to resolve and might add pressure to already heavy workloads (10,160).
Summary: Staffing shortages in maternity services (159)
- There is a well-recognised national shortage of maternity staff. Although staff are doing their best to deliver care, they are ‘stretched to the absolute limit’. The workforce is in ‘permanent crisis mode’ and staff shortages can mean that training gets cancelled. Some staff report concerns around quality of care and that some patient choices are being limited.
- Antenatal and postnatal care can be rushed due to pressures on staff time; and class closures and cancellations are common. This increases the likelihood of professionals missing important information from patients, such as mental health conditions or domestic abuse.
- Staffing pressures can have a substantial impact on staff morale and mental health; and lead to high levels of stress, exhaustion and burnout. This has led to a ‘vicious circle’ in many NHS trusts, where difficulties in retaining staff make conditions worse for remaining colleagues.
- Families using maternity services report that services can seem overwhelmed, and that staffing shortages can directly impact the quality of care they received. A survey of over 1,200 people who had given birth between August 2021 and July 2022 found that 1 in 3 had experienced delays in seeing a midwife, receiving pain relief, getting a prescription or being referred to other services.
Local picture
Local maternity services are provided by The Rosie Hospital in Cambridge; Hinchingbrooke Hospital in Huntingdon; and Peterborough City Hospital in Peterborough. Some families in Wisbech are served by Queen Elizabeth Hospital, which is located outside of Cambridgeshire and Peterborough.
All hospitals offer a listening and debriefing service for families who have had traumatic birth experiences, however only The Rosie Hospital provides specific support around birth choices (ensuring that birth experiences are as personalised and as safe as possible).

Table 11: Support services offered at local maternity services. Data source: (151)
The percentage of women and birthing people who have their booking appointment with a midwife within 10 weeks of their pregnancy was significantly above the national rates in Cambridgeshire and Peterborough in 2018/19 (15). The rate was higher in Cambridgeshire than in Peterborough.
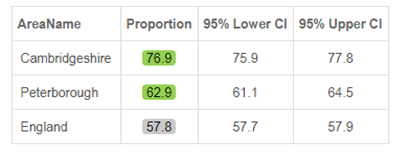
Table 12: Early access to maternity care, 2018/19. Data source: Fingertips
Workforce
The total number of midwives employed by CUH was similar in 2020 and 2022 (161).
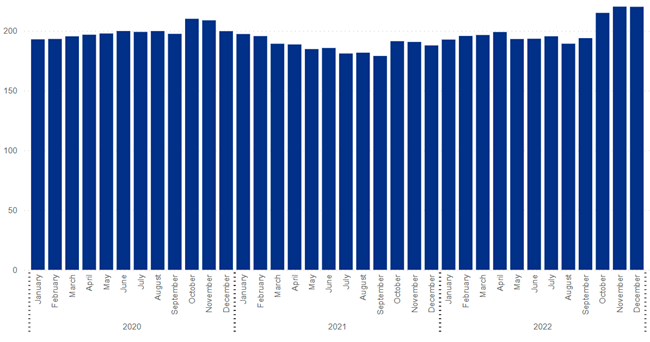
Figure 33: Number of full time equivalent (FTE) midwives employed by CUH, 2020 – 22. 1.0 FTE equates to full-time work of 37.5 hours per week. Image source: NHS Digital
There was a 14% reduction in the number of midwives employed by NWAFT in 2022, compared to 2020 (161).
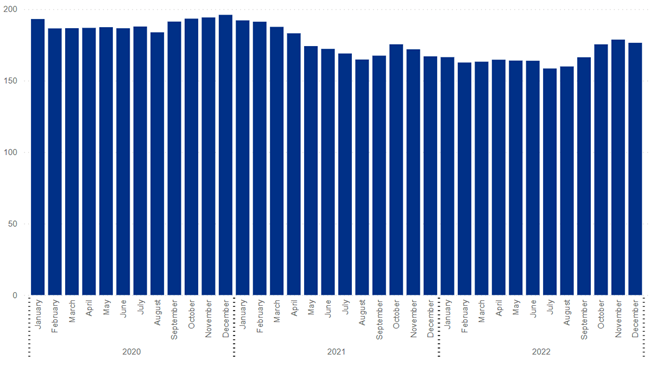
Figure 34: Number of full time equivalent (FTE) midwives employed by NWAFT, 2020 – 2022. 1.0 FTE equates to full-time work of 37.5 hours per week. Image source: NHS Digital
Experiences of services
The 2022 Maternity Services Survey found that North West Anglia NHS Foundation Trust (NWAFT), which covers Peterborough City Hospital and Hinchingbrooke Hospital, had below average scores for questions relating to antenatal and postnatal mental health support (162). The Care Quality Commission invited people to participate in this survey if they had a live birth during February 2022. It had 232 responses from CUH and 185 from NWAFT, a 57% and 42% response rate respectively.
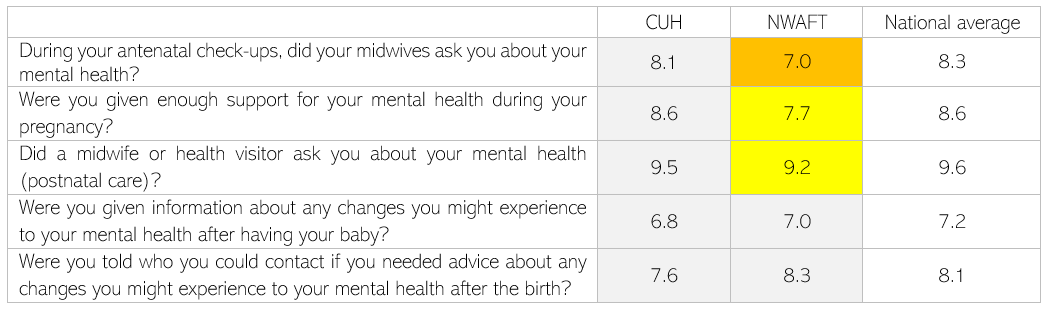
Table 13: Results of the NHS Maternity Services Survey 2022 for Cambridge University Hospitals (CUH) and North West Anglia NHS Foundation Trust (NWAFT). Data source: (162). Note: CUH covers The Rosie Hospital and NWAFT covers Peterborough City Hospital and Hinchingbrooke Hospital. Scores are given between 0 and 10, where 10 indicates the most positive patient experiences possible and 0 considerable room for improvement. Grey indicates results are similar to the national average, yellow that they are ‘somewhat worse than expected’ and orange that they are ‘worse than expected’.
A survey carried out by Rosie Maternity and Neonatal Voices found that (120):
- The majority of respondents reported having some kind of mental health concern (68%), but only 7% had a mental health diagnosis. 37% of respondents reported having mental health issues in the past; and 14% experienced mental health difficulties for the first time in the perinatal period.
- Over half of people had not received perinatal mental health support (58%), the majority of whom (74%) were interested in finding out about available support. This suggests a lack of awareness of what support is available. For those who did access mental health support:
- 47% found it hard to find out about support.
- 39% found it hard to access support.
- 86% found the support was helpful.
- Community midwives and GPs were the channels through which most respondents initially sought help with their mental health. Almost all respondents felt that perinatal mental health support could be better promoted, particularly within their maternity and discharge packs, and on The Rosie Hospital website.
- The majority of respondents felt that they needed more support to manage their anxiety around pregnancy and parenting (including breast feeding), which could impact their mental health.
- Remote support such as telephone counselling was seen as the most sought after by respondents. In general, having an open discourse about their mental health was important, and some felt that talking about their mental health should be part of appointments. The main issues people wanted support with were general depressive feelings, anxiety, loneliness and birth trauma.
- Note that a range of actions have been completed in response to this survey, including the addition of information about perinatal mental health on The Rosie Hospital website.
Healthy Child Programme
The Healthy Child Programme is run by a multi-disciplinary team of health visitors, nursery nurses and assistant practitioners, who provide community support for infants and children aged 0-5. As part of this programme, all families with babies should be offered 5 mandated health visitor reviews before their child is 2.5 years old (163). The Healthy Child programme is based on the principle of proportionate universalism, so provides a mix of universal and targeted provision.
- Health visitors provide support to all new parents and play a key role in recognising mental health problems and referring to specialist care, particularly during the 6-8 weeks visit post-birth. They aim to improve health outcomes and reduce inequalities across 6 areas (164).
Figure 35: 6 areas of support provided by health visitors. Adapted from: (164)
- Specialist health visitors have additional training in perinatal mental health. They can provide direct support to families, work with and provide referrals to specialist mental health services, and provide training and support for other health visitors (165).
- Nationally, the health visitor workforce has decreased by over a third since 2015 (166). There is an estimated shortfall of 5,000 health visitors in England; and 48% intend to leave the profession within the next 5 years (167).
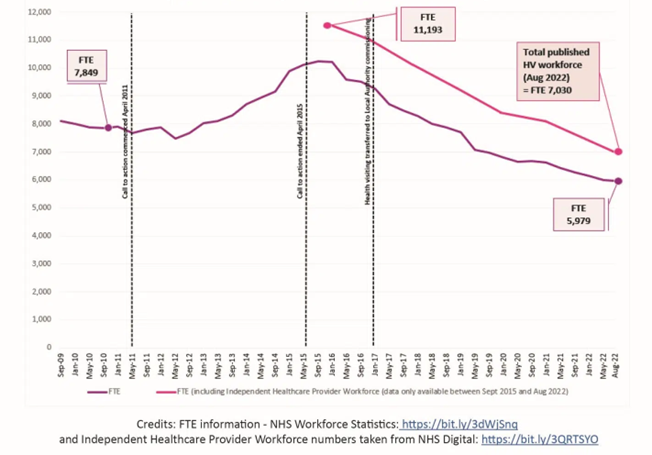
Figure 36: Size of the health visitor workforce from September 2019 to August 2022. Image source: Institute of Health Visiting
- Health visitors across the UK report that staff numbers are the biggest barriers to making a difference to families (167). A 2022 survey of health visitors found that (167):
- 86% reported there is not enough capacity in other services to pick up onward referrals, which is a key driver in families being left without support.
- 35% believed that the services they provided were inaccessible for some families.
- 70% felt ‘worried, tense or anxious’.
- A 2019 survey of 1000 mothers in England found that 22% felt that their interactions with health visitors felt like a ‘tick box exercise’. Key drivers for this were: lack of continuity of care, appointments feeling rushed, and difficulties accessing services when needed (168).
Local picture
- The proportion of 6 – 8 week and 2.5 year reviews carried out by health visitors is substantially lower than the national average in Cambridgeshire and Peterborough (169). Due to ongoing workforce and capacity issues, the local timeframe of new born visits and the 6 – 8 week reviews has been extended to up to 21 days and 12 weeks respectively.
- Average national rates for 2020/21 were:
- New born visits: 88% within the target timeframe of 14 days.
- 6-8 weeks review: 80% within the target timeframe of 8 weeks.
- 12 month review: 66% within the target timeframe of 12 months.
- 2.5 years review: 72% within the target timeframe of 2.5 years.
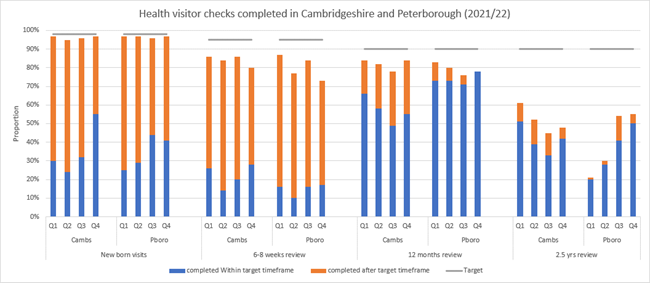
Figure 37: Health visitor service delivery metrics in Cambridgeshire and Peterborough in 2021/22. Data source: (169)
Experiences of services
Feedback on health visitors collated by the SUN network includes both positive and negative reports. This may reflect that local voices were collected across different areas of Cambridgeshire and Peterborough.
- Some people felt very supported by health visitors in terms of their mental health and being helped to access services; and felt that there was increasing awareness of perinatal mental health.
- Others felt that health visitors were ‘so overworked they are unable to focus on what is being said’.
- Some people felt that health visitors should be more knowledgeable about services they could signpost people to; or that they were unable to access mental health support as they did not meet strict service thresholds.
- Checks can sometimes carried out over the phone due to lack of resource, and weigh-ins are now ‘self-weigh-ins’. This can mean that people do not always have someone to answer their questions.
Feedback received from CPSL Mind who run groups, courses and offer 1:1 support in the community to address low or moderate mental health issues found that:
- Women often express their worries and dissatisfaction about the support received from health visitors including issues such as never meeting their health visitors in person as appointments are offered over the phone, or not having a named health visitor.
- Opportunities to identify women who suffer with mental health issues are missed as some women report lack of trust and/or difficulty in opening up about their mental health struggles to a health visitor that they did not have the opportunity to build a trusting relationship with.
- Feedback from women who also have older children highlighted that the care currently being offered since the start of the COVID-19 pandemic, is very different from the care they received pre-pandemic. Many women reported how useful the weigh-in clinics were in the past to get to know their health visitor and to build a trusting relationship over time. These presented regular opportunities for parents to talk about baby- and motherhood-related anxieties and get reassurances from their health visitor. These opportunities now don’t exist as clinics are only offered as ‘self-weigh-ins’ without the opportunity to talk to a professional about any issues parents may have.
An online survey carried out in May 2023 by Cambridgeshire Child and Family Centres (186) reported that only less than half (46%) of local parents would go to their health visitor or midwife if they were feeling low in the perinatal period.
Early Years services
Early Years services provide support to children and families, including baby groups and support with infant feeding. Co-location of services may help facilitate interprofessional collaboration (170).
Local picture
There are a range of Child and Family Centres across Cambridgeshire and Peterborough, all of which offer opportunities to meet other parents, and to access a range of information and support. This includes baby groups, young parents groups, self-weigh services, and breastfeeding support. Each child and family centre has its own Facebook page:
- South Cambridgeshire Child and Family Centres
- East Cambs Child and Family Centres
- Cambridge City Child and Family Centre
- Wisbech Child & Family Centres
- Huntingdonshire Child and Family Centres
- East and First Steps C&FCs – Central and East Peterborough
- Honeyhill C&FC – North West and Rural Peterborough
- Orton C&FC – South Peterborough
- March, Chatteris & Whittlesey C&FCs – South Fenland
Since 2010, there has been a 30% reduction in the number of children’s centres in Cambridgeshire; and a 53% reduction in the number of children’s centres in Peterborough (66).
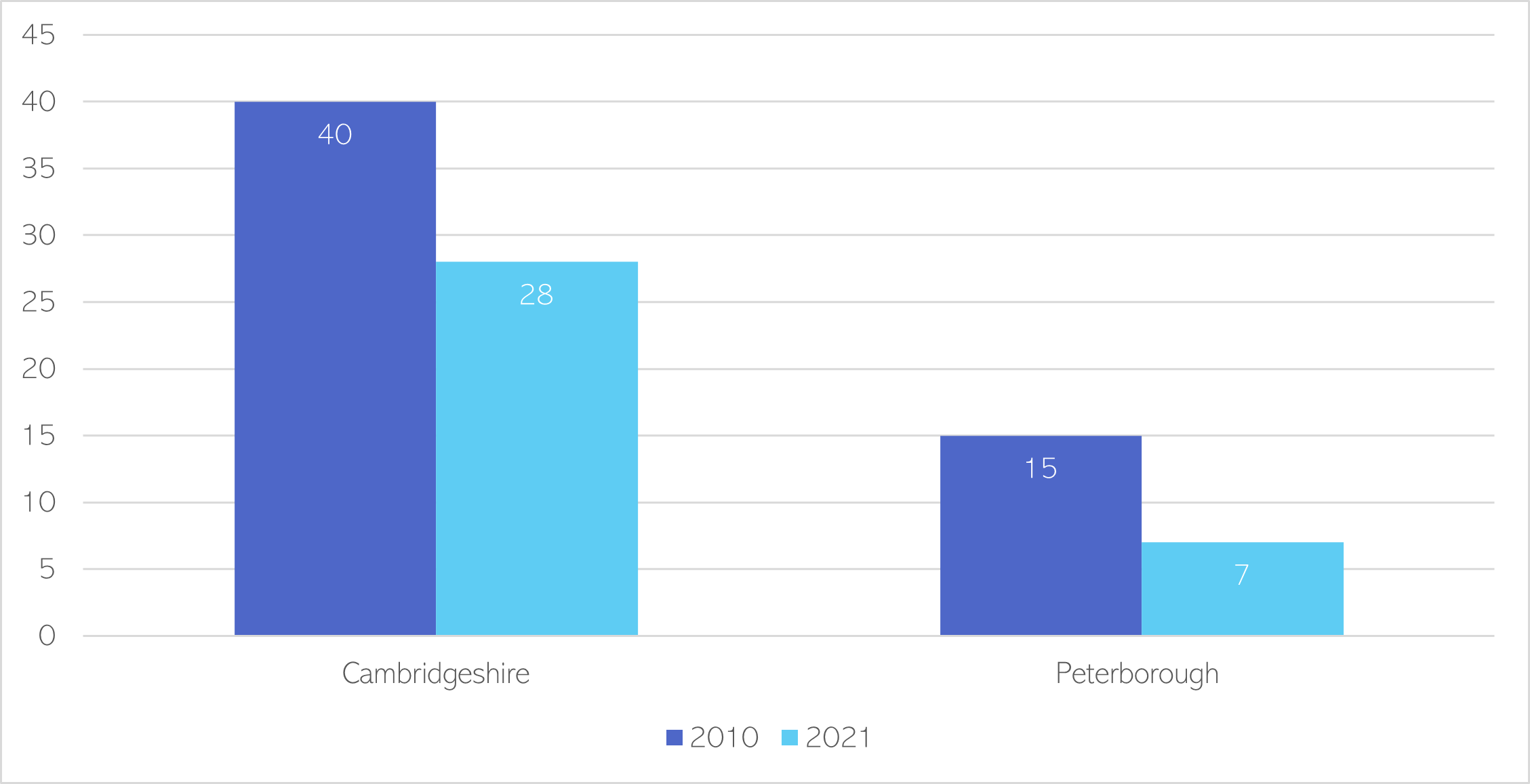
Figure 38: Number of children’s centres in Cambridgeshire and Peterborough in 2010 and 2021. Data source: (66)
There has recently been investment in Family Hubs. Initial funding was for Peterborough (171), but they are also being developed in Cambridgeshire.
- Family Hubs will use a whole family approach to offer a single access point to family support services.
- They will be integrated across the wider system, including voluntary and community organisations, education settings and health and social care.
- They will offer support to families, from conception to 19 years, or up to 25 years for young people with special educational needs and disabilities (SEND).
- A large proportion (31%) of Family Hubs funding will be used to improve perinatal mental health and parent-infant relationships.
Cambridgeshire Child and Family Centres are mostly used by mothers and female carers. To understand how to better engage men in their services they ran an online survey for men in November 2022. The survey was distributed on the Centres’ Facebook pages and received 180 replies (186).
- 51% did not know about the types of activities and services offered by Child and Family Centres
- Only 12% knew about general support and signposting around mental health, domestic abuse, and money offered by Child and Family Centres
- 62% said they would like more information and support about how they as a fathers or male carers can support their child(ren)’s development and wellbeing.
- 59% said that they would like to have opportunities to have face to face activities and support specifically for men and their children and indicated a strong preference for these activities to be offered outside of working hours, especially during the weekend.
- The survey also looked at whether men felt involved if the family received support through a family worker and identified that 33% of men did not feel involved.
- Most respondents spoke highly about family workers who were great at involving the men as well as the mother in the support given to the family, but also highlighted that some family workers only focused on the mother and in some cases the men felt excluded. One respondent said: “it is very aimed at the mother which in my situation I understand as my children’s mother is at home with them and I am working. However I am still involved and when we had these visits it would be good to check in on dad as well’.
Additional resources
- NICE Guidelines on antenatal and postnatal mental health
- Supporting mental healthcare in a maternity and neonatal setting: Good practice guide and case studies
- A good practice guide to support implementation of trauma-informed care in the perinatal period
- Standards for Community Perinatal Mental Health Services
- Why Health Visitors Matter: Perspectives on a widely valued service
- What works to enhance the effectiveness of the Healthy Child Programme: An evidence update
References
Full list of references can be accessed here.
- Maternal Mental Health Alliance. Defining essential perinatal mental health care: maternity services [Internet]. 2023 [cited 2023 Feb 16]. Available from: https://maternalmentalhealthalliance.org/campaign/make-all-care-count/maternity-services/
- World Health Organisation. Newborns: improving survival and well-being [Internet]. 2020 [cited 2023 Feb 17]. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality
- Rayment-Jones H, Harris J, Harden A, Khan Z, Sandall J. How do women with social risk factors experience United Kingdom maternity care? A realist synthesis. Birth. 2019;46(3).
- Baby Loss and Maternity All Party Parliamentary Groups. Safe Staffing: The impact of staffing shortages in maternity and neonatal care [Internet]. 2022 [cited 2023 Feb 9]. Available from: https://www.sands.org.uk/sites/default/files/Staffing%20shortages%20-%20APPG%20report,%20Oct%2022%20(final).pdf
- McGlone C, Hollins Martin CJ, Furber C. Midwives’ experiences of asking the Whooley questions to assess current mental health: a qualitative interpretive study. J Reprod Infant Psychol. 2016;34(4).
- NHS Digital. NHS Workforce Statistics – December 2022 (Including selected provisional statistics for January 2023) [Delayed from 30/03/23] [Internet]. NHS workforce statistics. 2023 [cited 2023 Apr 19]. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-workforce-statistics/december-2022
- Care Quality Commission. NHS Maternity Services Survey 2022 Benchmark Report: Cambridge University Hospitals NHS Foundation Trust [Internet]. 2022 [cited 2023 Feb 7]. Available from: https://nhssurveys.org/all-files/04-maternity/05-benchmarks-reports/2022/
- Public Health England. Improving public health outcomes for children, young people and families. Guide 1: Background information on commissioning and service model [Internet]. 2021 [cited 2023 Mar 10]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/969168/Commissioning_guide_1.pdf
- Duncan H. National Health Visitor Programme: Benefits Realisation. 2017.
- Health Education England. Specialist Health Visitors in Perinatal & Infant Mental Health [Internet]. 2016 [cited 2023 Feb 13]. Available from: https://www.hee.nhs.uk/our-work/specialist-health-visitors
- Institute of Health Visiting. Health visitor workforce numbers in England reach an all-time low [Internet]. 2022 [cited 2023 Feb 10]. Available from: https://ihv.org.uk/news-and-views/news/health-visitor-workforce-numbers-in-england-reach-an-all-time-low/
- Institute of Health Visiting. State of Health Visiting, UK survey report [Internet]. 2023 [cited 2023 Feb 13]. Available from: https://ihv.org.uk/wp-content/uploads/2023/01/State-of-Health-Visiting-Report-2022-FINAL-VERSION-13.01.23.pdf
- Institute of Health Visiting. Health Visiting in England: A Vision for the Future [Internet]. 2019 [cited 2023 Feb 10]. Available from: https://ihv.org.uk/wp-content/uploads/2019/11/7.11.19-Health-Visiting-in-England-Vision-FINAL-VERSION.pdf
- Office for Health Improvement and Disparities. Health visitor service delivery metrics experimental statistics: annual data 2021 to 2022 [Internet]. 2022 [cited 2023 Feb 13]. Available from: https://www.gov.uk/government/statistics/health-visitor-service-delivery-metrics-experimental-statistics-annual-data-2021-to-2022
- Olander EK, Aquino MRJ, Bryar R. Three perspectives on the co-location of maternity services: qualitative interviews with mothers, midwives and health visitors. J Interprof Care. 2020;