Specialist perinatal mental health services
Specialist perinatal mental health services support people with severe or complex perinatal mental health needs (176). This includes those with chronic difficulties which may be exacerbated by the perinatal period, or those experiencing an onset of difficulties during this time.
- Specialist perinatal mental health services can advise people with pre-existing mental health conditions to help them make informed decisions around pregnancy, birth plans and postnatal care (176). They also provide advice about the management of pre-existing mental health conditions during the perinatal period, medication in pregnancy and breastfeeding, and the risk of postpartum recurrence of illness (21).
- It has been recommended that specialist perinatal mental health teams are available to everyone, regardless of location. However, the patchy provision of services is a national issue (177).
- The NHS Long Term Plan states that services should assess the mental health of people whose partners are accessing specialist perinatal mental health services, and should signpost them to support (178). Services should ‘think family’ and involve partners and other family members in care (33).

Figure 41: 3 underpinning principles (outer ring) and 10 key ideas (inner ring) for good practice when involving and supporting partners and families in specialist perinatal mental health services. Image source: Involving and supporting partners and other family members in specialist perinatal mental health services: Good practice guide
Psychotropic medication and perinatal mental health
- Many women and birthing people receiving treatment for mental health conditions with psychotropic medication become pregnant. A large proportion end up stopping taking medication during their pregnancy (179).
- Continuation of medication during pregnancy is a protective factor against illness relapse for women with serious mental illness (180).
- NICE guidelines highlight that healthcare professionals should take into account individual needs and preferences around prescriptions, and work in partnership with patients to support them to make informed decisions about their treatment (110).
- A review of qualitative research highlights that whilst many women do not feel empowered to make decisions about the use of antidepressants during pregnancy, they often want to be involved in collaborative decision-making about antidepressant use (181).
- This toolkit provides a best practice guide for the provision of pre-conception advice by perinatal mental health services.
Maternal mental health services
Maternal mental health services combine maternity, reproductive health and psychological support for women and birthing people who experience moderate and severe or complex mental health needs, which arise from/are related to their maternity experience (182). This includes parents who: develop PTSD following birth trauma, experience perinatal loss and tokophobia (severe fear of childbirth), and experience loss through separation (custody loss) (182).
Alongside the strong compassionate argument for these services, there is a strong economic case for the provision of specialist counselling for parents who experience baby loss. These services have been shown to produce £2.71 savings for every £1 investment (188). Savings arise as the costs of unresolved trauma are high in terms of health care and benefits payments (188).
Local picture
There are two hospital-based maternity clinics in Cambridgeshire and Peterborough. In addition, The Rainbow Clinic at The Rosie Hospital provides specialist care and support to families who have experienced the death of a baby during pregnancy or shortly afterwards, during their next pregnancy. Hospital-based maternity clinics in Cambridgeshire and Peterborough currently provide (151):
- Maternal Wellbeing Clinic (The Rosie Hospital): An obstetrician run clinic, that supports women antenatally with mental health concerns. Provides advice and support throughout pregnancy regarding mental health, by offering pre-birth planning meetings, supporting birth plans, and signposting to mental health services. This includes advice about medication during pregnancy and breastfeeding.
- Sunflower Clinic (Peterborough City and Hichingbrooke Hospital): Provides mental health support for antenatal patients who are identified by their community midwives as having a serious mental health problem or needing additional support with their mental health during pregnancy.
A new Maternal Mental Health Service is awaiting funding, which will provide support for people with severe mental health difficulties in the context of perinatal loss, birth trauma, tokophobia and custody loss. This service will cover Cambridgeshire and Peterborough but is currently not developed, leaving gaps in NHS provision. Note that Ormiston Families MPower provide a person-centred supportive service to women who have experienced recurrent custody loss. They are active in Fenland and currently launching in Peterborough.
Specialist perinatal mental health team
Specialist community perinatal mental health teams provide support for people with severe or complex mental health needs during the perinatal period (176). NICE guidelines for perinatal mental health highlight that assessments for treatment should take place within 2 weeks of referral; and that psychological interventions should be provided within 1 month of initial assessment (183).
Local picture
The Cambridgeshire and Peterborough NHS Foundation Trust (CPFT) specialist perinatal mental health team is a team of mental health specialists helping women and birthing people with serious and complex mental health conditions during pregnancy and up to a year after birth, including pre-conception counselling and support around birth trauma (151). It opened in February 2019 and provides support across Cambridgeshire and Peterborough.
Occupational Therapists (OTs) within the Perinatal Team offer individual and group intervention work. They focus work on identity and role transitions during the perinatal period, support with routine and occupational balance, advice around co-occupations – this may include play, feeding and sleeping, sensory needs assessments, community integration and education for both the individual and their significant others. They also complete intervention to support women back to work or education settings. An individual may be allocated an OT to work with during their time with the team or can be referred for 1:1 or group support.
The perinatal mental health survey (118) carried out with over 200 mothers by Rosie Maternity and Neonatal Voices identified that:
- 3% of respondents wanted birth trauma and/or anxieties around neonatal care be addressed. This was the 5th highest ranking mental health issue identified by the survey.
- More respondents wanted high-level mental health support than had sought help. High level was described as ‘planned series of counselling with regular follow ups/ monitoring from professionals.’ Most service users who accessed support from the specialist perinatal mental health team had found this support beneficial.
Progress towards NHS Long Term Plan
The current progress towards NHS Long Term plan ambitions for perinatal mental health are mixed as of May 2023, with the least progress being made towards the provision of support for fathers and partners. Progress towards the ambitions of the NHS Long Term Plan in May 2023 (as defined in Specialist perinatal mental health care in the UK 2023) was that:
- Ambition that specialist perinatal mental health services providing care from pre-conception to 24 months after birth: budget and start data agreed, but service is not currently being delivered
- Ambition that specialist perinatal mental health services seeing increasing number of women, including those with complex post-traumatic stress disorder (c-PTSD) /personality disorder diagnosis: service is currently being delivered
- Ambition that specialist perinatal mental health services offering sufficient psychological therapies including parent-infant, couple, co-parenting and family interventions: budget and start data agreed, but service is not currently being delivered
- Ambition that specialist perinatal mental health services offering fathers/partners assessment for their mental health and signposting for support: service not currently offered. No funding and start date agreed.
Annual peer review
A review carried out in December 2022 found that this service:
- Had a strong multi-disciplinary team, which provided a wide range of support services.
- Had good links with a number of partner agencies, including maternity services, Talking Therapies and voluntary sector organisations.
- Was described as a ‘lifeline’ by a small sample of mothers who had used this service.
- Faced issues with inadequate estates provision and technical difficulties with SystemOne; and was struggling to meet their access rates target (see slides for further details). Recruitment to some posts (including psychiatrists and nurses) was also challenging.
Access rates
In 2016, the initial target for access to this service covered 10% of births (1,056). As the expected increase in funding did not come through to the services, the target was adjusted to 728 for 2022/23. The current access rate is 670 as of April 2023.
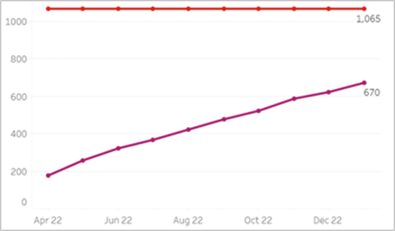
Figure 42: Cumulative year to date access from April 2022 and 22/23 target, Cambridgeshire and Peterborough ICB. Source: NHSFutures, Perinatal Mental Health Dashboard
Mother and Baby Units
Mother and baby units (MBUs) provide inpatient mental healthcare for people with severe postnatal mental health conditions, allowing parents and babies (and sometimes other family members) to stay together (176).
- MBUs are recommended in 2014 NICE guidelines and aim to facilitate mother-infant relationships (110).
- Separation of parents and infants resulting from inpatient mental healthcare causes significant distress; and can prevent breastfeeding and the early development of mother-infant relationships (21).
- A national evaluation comparing MBUs to other types of inpatient mental healthcare found that whilst there was no difference in readmission rates; satisfaction with care was significantly greater for people admitted to MBUs (184). Women and clinicians feel that MBUs provide more family-centred care than general wards, in which separation from babies can be a traumatic experience that is detrimental to recovery (185).
Local picture
The specialist perinatal mental health team has strong links with regional MBUs, including the locally commissioned Kingfisher Unit based in Norwich. Although there are no MBUs within Cambridgeshire and Peterborough (186), the specialist perinatal health team is able to provide intensive support for some women who refuse voluntary admission to MBUs (which may be due to distance).

Figure 43: Location of MBUs in England. Map created by Action of Postpartum Psychosis. Image source: Google Maps
Additional resources
- Guidance for commissioners of perinatal mental health services
- NICE Guidelines on antenatal and postnatal mental health and pregnancy and complex social factors: a model for service provision for pregnant women with complex social factors
- Royal College of Psychiatrists report Perinatal mental health services: Recommendations for the provision of services for childbearing women
- Occupational therapy and perinatal mental health and a blog about an occupational therapist working in perinatal care
- A good practice guide to support implementation of trauma-informed care in the perinatal period
- Standards for Inpatient Perinatal Mental Health Services
- Specialist perinatal mental health care in the UK 2023
- Involving and supporting partners and other family members in specialist perinatal mental health services: good practice guide
- Guide for delivering preconception care to women with a serious mental illness
- Implementing Routine Outcome Monitoring in Specialist Perinatal Mental Health Services
- Life after loss: An economic evaluation of specialist counselling after baby loss
References
Full list of references can be accessed here.
- Maternal Mental Health Alliance. Defining essential perinatal mental health (PMH) care: specialist PMH services [Internet]. 2023 [cited 2023 Feb 16]. Available from: https://maternalmentalhealthalliance.org/campaign/make-all-care-count/specialist-perinatal-mental-health-services/
- Maternal Mental Health Alliance. Community specialist perinatal mental health teams [Internet]. 2023 [cited 2023 Feb 7]. Available from: https://maternalmentalhealthalliance.org/campaign/act-now/community/
- NHS. NHS Long Term Plan [Internet]. 2019 [cited 2023 Feb 8]. Available from: https://www.longtermplan.nhs.uk/
- Petersen I, Gilbert RE, Evans SJW, Man SL, Nazareth I. Pregnancy as a major determinant for discontinuation of antidepressants: An analysis of data from The Health Improvement Network. Journal of Clinical Psychiatry. 2011;72(7).
- Taylor CL, Broadbent M, Khondoker M, Stewart RJ, Howard LM. Predictors of severe relapse in pregnant women with psychotic or bipolar disorders. J Psychiatr Res. 2018;104.
- Randall L, Briscoe L. Are women empowered to make decisions about the use of antidepressants in pregnancy? Vol. 26, British Journal of Midwifery. 2018.
- NHS England. Maternal mental health services [Internet]. 2023 [cited 2023 Feb 28]. Available from: https://www.england.nhs.uk/mental-health/perinatal/maternal-mental-health-services/
- NICE. Antenatal and postnatal mental health: clinical management and service guidance. Essentially MIDIRS. 2015;6(1).
- Howard LM, Trevillion K, Potts L, Heslin M, Pickles A, Byford S, et al. Effectiveness and cost-effectiveness of psychiatric mother and baby units: quasi-experimental study. British Journal of Psychiatry. 2022 Oct 21;221(4):628–36.
- Griffiths J, Lever Taylor B, Morant N, Bick D, Howard LM, Seneviratne G, et al. A qualitative comparison of experiences of specialist mother and baby units versus general psychiatric wards. BMC Psychiatry. 2019;19(1).
- Maternal Mental Health Alliance. Accredited Mother and Baby Units [Internet]. 2021 [cited 2023 Feb 7]. Available from: https://maternalmentalhealthalliance.org/wp-content/uploads/mother-and-baby-units-map-united-kingdom-MMHA-April-2021.pdf