What is the link between diet, weight and mental health?
- Eating a balanced diet can have positive impacts on mental as well as physical health (NHS England, 2016a). For example:
- Higher fruit and vegetable consumption is associated with greater mental wellbeing (Stranges et al., 2014).
- Diets which are heavily based on processed foods, refined carbohydrates and saturated fats are associated with poorer mental health in children and young people, with particularly strong links with depression and anxiety (O’Neil et al., 2014).
- There is a bidirectional relationship between poor mental health and obesity:
- Weight gain often has negative impacts of individuals’ self-esteem and quality of life (J. Firth et al., 2019).
- People who have depression are more likely to develop obesity, and vice versa (Rajan & Menon, 2017).
- There are also strong associations between obesity and anxiety, as well as obesity and eating disorders (Rajan & Menon, 2017).
- Evidence suggests that there are many common risk factors for eating disorders and obesity, ranging from individual factors, to wider societal factors (Haines & Neumark-Sztainer, 2006; Sánchez-Carracedo et al., 2012).
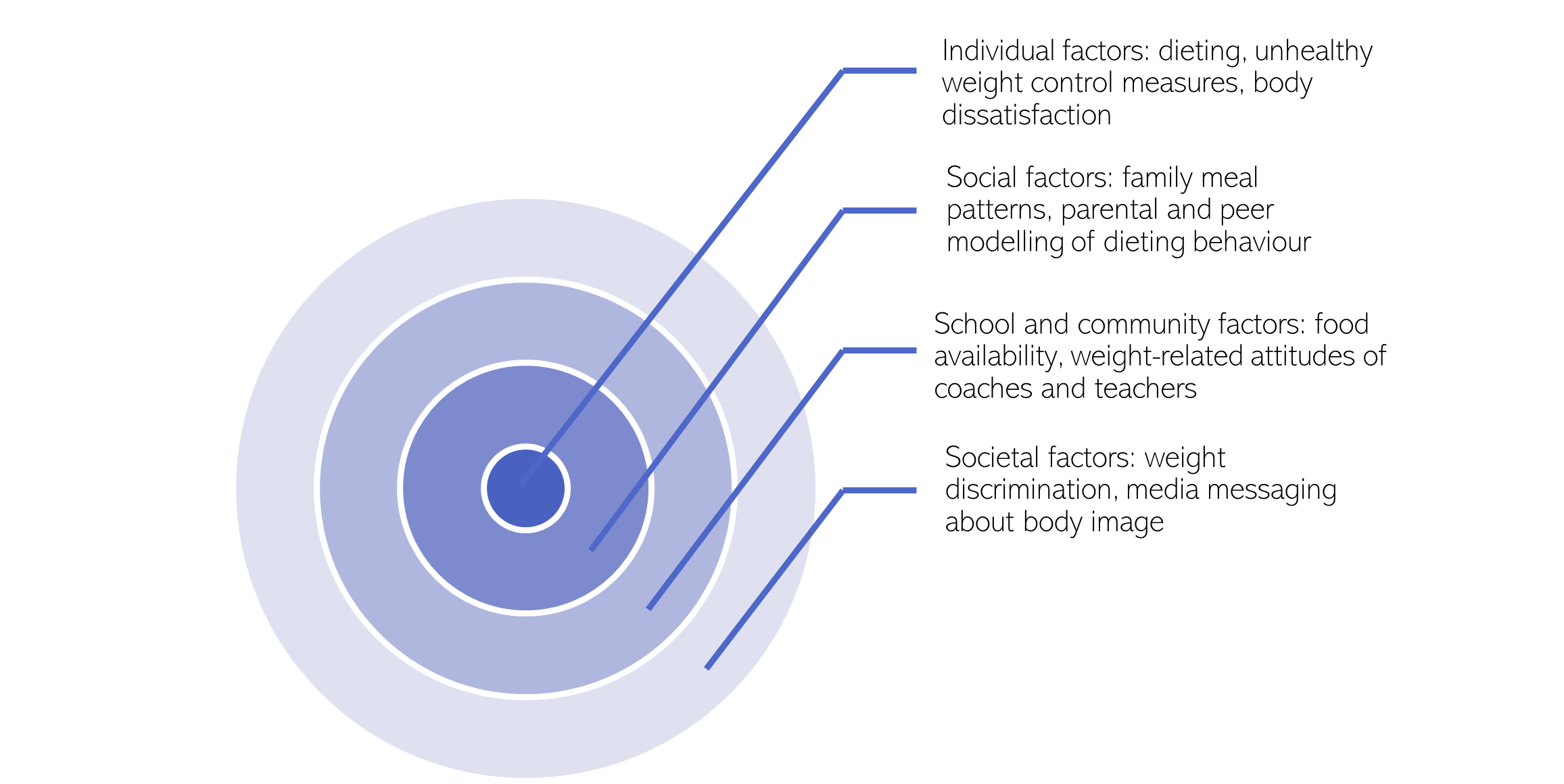
Figure 88: Common risk factors for eating disorders and obesity. Adapted from: (Sánchez-Carracedo et al., 2012)
People who have poor mental health are more likely to have a negative view of their bodies, with one survery finding that around a third feel shame (36%) and despair (31%) when looking at their body in the mirror (Ipsos MORI, 2021).
Why are some people with mental health conditions more likely to have a poor diet?
- There are common risk factors for mental health conditions and poor diets. For example, stressful life events are associated with changes in appetite and dietary preferences (J. Firth et al., 2020), and weight gain (Harding et al., 2014). They can also lead to the development of mental health conditions.
- Some antipsychotic medications and antidepressants increase in appetite and lethargy, and cause weight gain (J. Firth et al., 2019). The weight gain caused by psychotropic medication often has a negative impact on people’s quality of life of people and contributes to medication non-adherence (Mccloughen & Foster, 2011).
- Poor diets can increase risk of physical health conditions, which are risk factors for mental health conditions. For example, diets with a high glycaemic index are a risk factor for type 2 diabetes, which is associated with depression (J. Firth et al., 2020).
- People with mental health conditions are disproportionately likely to face barriers to maintaining a healthy diet (J. Firth et al., 2020).
- People with severe mental illnesses report (Wilton, 2020):
- Finding it difficult to stay motivated to eat healthily as their mental health fluctuates.
- Complicated relationships between their diet and their emotions.
- A lack of long-term support from services to maintain a healthy weight.
Poverty and deprivation
The Marmot Review highlights that solely focusing on health behaviours is unlikely to reduce health inequalities (Marmot & Bell, 2012). Instead, we need to take a system-level approach, and consider how socioeconomic factors such as poverty impact physical and mental health.
Table 32: Links between poverty, deprivation, and mental physical health.
| Common risk factors | Links with mental health |
| Food poverty is a common risk factor mental health conditions, poor quality diets and obesity |
|
| Poor mental health, poor diets and obesity cluster in highly deprived neighbourhoods |
|
What is the national picture?
- There are strong associations between some mental health conditions and quality diets:
- People experiencing major depression have poorer quality diets than those in the general population (J. Firth et al., 2019).
- Similarly, people with serious mental illness have poorer quality diets than the general population. This trend is present even after adjusting for social deprivation (J. Firth et al., 2019).
- People who are clinically underweight or obese are most likely to report poor mental health (Ipsos MORI, 2021)
- Stressors related to the COVID-19 pandemic have been linked to poor mental health and unhealthy behaviours, such as poor-quality diets (Melamed et al., 2022).
Links between body image and mental health (Mental Health Foundation, 2019)
- Body satisfaction is associated with higher wellbeing, whilst body dissatisfaction is associated with poorer quality of life, and an increased risk of depression and eating disorders.
- People of all ages are impacted by poor body image:
- 1 in 5 adults, and almost 1 in 3 teenagers, have felt shame because of their body image in the past year.
- 1 in 8 adults have experienced suicidal thoughts because of concerns about their body image.
- 10% of boys in secondary school have skipped a meal to change their appearance.
- Body image can be influenced by:
- Interpersonal relationships, including relationships with family and friends, how families and peers speak about bodies and appearance.
- LGBTQ+ people and those with chronic illnesses are at higher risk of poor body image.
What is the local picture?
The proportion of adults classified as overweight or obese is varies significantly over Cambridgeshire and Peterborough (Office for Health Improvement and Disparities, 2023):
- The proportion of adults classified as overweight or obese is lower than the national average in Cambridge and South Cambridgeshire.
- The percentage of adults who are classified as overweight or obese in 2020/21 was highest is Fenland (67.1%), though this was a substantial decline compared to the previous year (74.6%).
- 5% of adults in East Cambridgeshire were classified as overweight or obese in 2020/21, an increase compared to 57% in 2019/20.
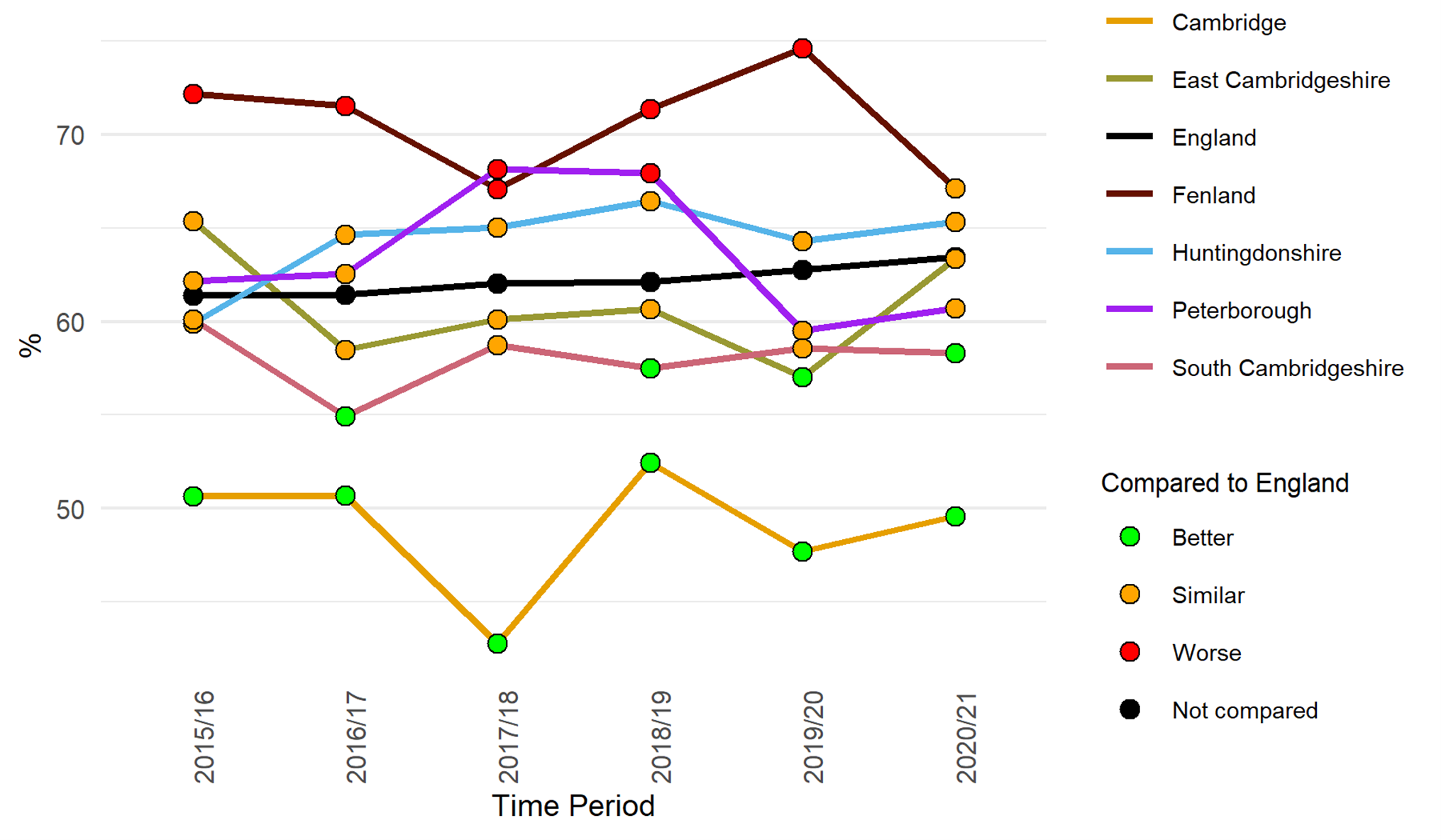
Figure 89: Percentage of adults (aged 18+) classified as overweight or obese. Data source: Fingertips
In 2021/22, the proportion of 10 to 11-year-olds who are classified as overweight or obese in Peterborough (41.2%) was significantly higher than the national rate (37.8%). The proportion in other areas of Cambridgeshire and Peterborough was close to or lower than the national rate (Office for Health Improvement and Disparities, 2023).

Figure 90: Proportion of children aged 10 to 11 years classified as overweight or obese. Data source: Fingertips. Note that data was not collected in 2020/21 due to COVID-19 restrictions.
Additional resources
- The local data pack gives an overview of key data and trends
- NIHR summary of how health behaviours are important to public mental health
- UK Parliament briefing on Diet-related health inequalities
- Food insecurity and severe mental illness: understanding the hidden problem and how to ask about food access during routine healthcare
- Obesity and Mental Health evidence review
- House of Commons report on The impact of body image on mental and physical health
References
Full list of references is included at the end of this chapter.