What is the link between physical activity and mental health?
- Physical activity can reduce mortality and improve life expectancy (NHS England, 2016a). Even small increases in levels of physical activity have health benefits (NHS England, 2016a).
- Physical activity can also act as a protective factor against a range of mental health conditions, including depression and anxiety; as well as reducing stress and improving self-esteem (Public Health England, 2019a). It has been estimated that 12% of depression cases could be prevented by people doing an hour of physical activity each week (Harvey et al., 2018).
- Supporting people with severe mental illness to become more physically active is a key priority for reducing health inequalities and improving overall quality of life in this group, by improving social inclusion and self-confidence [(Machaczek et al., 2022),(Soundy et al., 2014)].
- Aerobic exercise, such as walking or cycling, has been shown to improve mental health outcomes in people with schizophrenia and schizoaffective disorder (Stanton & Happell, 2014).
- Exercise interventions have also been shown to alleviate the secondary symptoms of schizophrenia, such as low self-esteem, social withdrawal and depression (Richardson et al., 2005).
Why are some people with mental health conditions less likely to be physically active?
People with severe and enduring mental health conditions are disproportionately excluded from participating in physical activity (Best et al., 2022). Barriers to people with SMI staying physically active include (Machaczek et al., 2022):
- Individual factors: severity of mental health symptoms, feeling too unwell, low energy, poor physical health, financial costs of physical activity, and a lack of self-confidence. For example, some adults with severe mental illnesses report feeling a sense of ‘powerlessness’ around improving their physical health (Schmutte et al., 2009).
- Organisational factors: ‘culture of sitting’ in inpatient mental health settings,
- Community factors: social isolation, lack of social support, lack of access to sports facilities, poor perceptions of neighbourhood safety.
- Policy factors: fear of being assessed as ‘fit for work’ and losing disability benefits.

Figure 80: Factors that impact the ability of people with severe mental illness to stay physically active. Adapted from: (Machaczek et al., 2022)
- These factors often interact with each other: for example, there is a higher prevalence of severe mental illness in more deprived areas (Public Health England, 2018c), which is linked to physical inactivity (Farrell et al., 2013).
- There is promising evidence showing that interventions encouraging people with severe mental illness to become physically active are effective (Best et al., 2022).
- Providing support, both social and practical (such as with transport), can help people engage with physical activity (Soundy et al., 2014).
- People with severe mental illness are no less likely to adhere to physical activity interventions than people in the general population (Richardson et al., 2005).
What is the national picture?
- 8% of women and 63.1% of men in England meet NHS recommended levels of physical activity (DCMS, 2022).
- Levels of physical activity vary by between ethnic groups (DCMS, 2022):
- People of mixed ethnic backgrounds are the most likely to be physically active, whilst people from Asian ethnic groups are least likely. This has been a consistent trend over the past 6 years.

Figure 81: Percentage of adult women (16+) classed as ‘physically active’, by ethnicity. Data source: Department for Digital, Culture, Media and Sport 2022
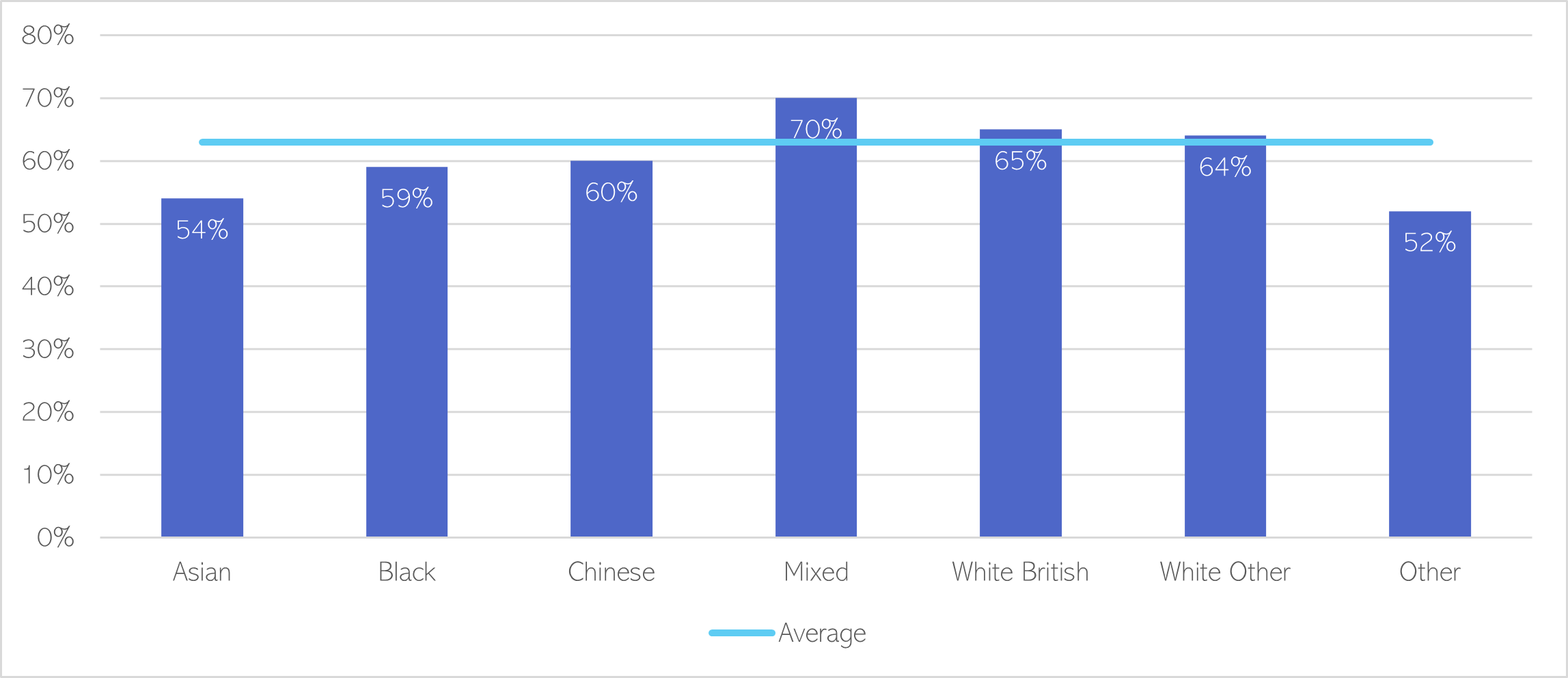
Figure 82: Percentage of adult men (16+) classed as ‘physically active’, by ethnicity. Data source: Department for Digital, Culture, Media and Sport 2022
- Disabled people are twice as likely to be inactive compared to their non-disabled peers (DSA UK & Activity Alliance, 2018). Key barriers disabled people face to engaging in physical activity include financial barriers and fear of having benefits sanctioned if seen being active (DSA UK & Activity Alliance, 2018).
- People with severe mental illnesses are much more likely to have a sedentary lifestyle compared to the general population. For example, adults with major depressive disorder generally have low levels of physical activity, with 2 in 3 not meeting recommended physical activity guidelines (Schuch et al., 2017).
What is the local picture?
For all districts other than Cambridge, the proportion of physically active adults decreased in 2020/21, compared to the previous year (Office for Health Improvement and Disparities, 2023).
- The proportion of physically active adults in Fenland (55.8%) and Peterborough (57.4%) is significantly lower than the national rate (65.9%). There has been a substantial decrease in the proportion of adults in Peterborough who report being physically active since 2018/19.
- The proportion of physically active adults is above average in Cambridge and East Cambridgeshire.

Figure 83: Percentage of adults (aged 19+) who meet NHS guidelines for physical activity. Data source: Fingertips
In 2020/21, the proportion of physically active children and young people declined compared to the previous year in Cambridgeshire. The data for Peterborough is not available for this time period. However, there was a steep decline in the proportion physically active children and young people in Peterborough (37.0%) in 2019/20, compared to the previous year (50.1%).

Figure 84: Percentage of physically active children and young people (5 – 16 yrs). Data source: Fingertips
The percentage of adults cycling for travel at least 3 days a week is 9 times higher than the national average in Cambridge. It is also above average in South Cambridgeshire and Cambridgeshire.

Table 31: Percentage of adults cycling for travel at least three days per week, 2019/20. Data source: Fingertips
Additional resources
- The local data pack gives an overview of key data and trends
- NIHR summary of how health behaviours are important to public mental health
- Mental Health Foundation report on Empowering people through physical activity
- A whole systems approach to integrating physical activity to aid mental health recovery in people with SMI
- Local data on physical activity levels
- Tools and evidence for supporting healthcare professionals to promote physical activity
References
Full list of references is included at the end of this chapter.