Risk and preventative factors
‘While older people may possess many protective factors for good mental health, they face numerous risk factors, including poorer physical health, reduced mobility and, for some, poverty and racism.’ (Centre for Mental Health & Age UK, 2024)
- Older people experience complex social, psychological and physical factors that influence the pattern, cause, diagnosis, treatment and prognosis of mental health conditions (Public Health England, 2019b). Often mental ill health results from a combination of factors, which may include the cumulative impact of poor mental health and adversity across someone’s life (Davidson, 2021).
- There are common risk factors for many different conditions (mental ill-health, physical ill-health, frailty and dementia) that impact older people. Supporting older adults to promote positive mental wellbeing (known as healthy ageing) therefore requires a whole system approach which addresses wider determinants of health, across local authorities, health and voluntary and community sector organisations (The Association of Directors of Public Health, 2018).
- Similarly, addressing the wider determinants of health is likely to be key to promoting good mental wellbeing. Older people (aged 50+) from a range of backgrounds identify health, social connections and financial security as key to happiness and a meaningful life (Centre for Ageing Better, 2015).
Case study: highlighting the impact of multimorbidity
The following anonymised case study gives an example of how multiple factors, including social issues and physical health needs, can impact older adults’ mental health and wellbeing.
- A woman ‘A’ in her mid-70s lives with her husband in Cambridgeshire and has children who live in a different area. A has a long history of recurrent depression which dates back over 40 years. She has received various treatment for this, including antidepressants and a course of cognitive behavioural therapy (CBT). Since 2018, she has had four inpatient admissions with a diagnosis of severe depression with psychosis under Section 2 and Section 3 of the Mental Health Act. She has also required several courses of electroconvulsive therapy (ECT).
- A is currently being supported by the community mental health team. She has intensive support from a community nurse, support worker, social worker and regular medical reviews. A currently does not feel like she will benefit from psychological support.
- A has a complex physical health history and has experienced both complications from ulcerative colitis and a hip fracture. She was recently transferred into general hospital for rehydration. She then had a fall whilst in hospital and sustained a fracture. A has issues with her heart relating to her antipsychotic medication, which have led her medications to be changed. On top of this, she has repeatedly experienced urinary tract infections (UTIs). This has led to her experiencing delirium and later relapses of depression.
- Since getting a colostomy bag, A has been reluctant to engage in activities that might help support her mental wellbeing such as going to church, walking and meeting friends. She prefers to stay indoors as she is worried that she might not have facilities to empty her colostomy bag, which has had a negative impact on her self-esteem and confidence.
Focus: Dementia prevention
Between 1991 and 2011 the Cognitive Function and Ageing Studies (CFAS) examined changes in dementia occurrence across 20 years in the UK. In both 1991 (CFAS I) and 2011 (CFAS II) studies, population-representative samples of over 7,500 older people were recruited, using almost identical methodology. Prevalence rates of dementia were calculated for men and women in 5-year age-bands. By applying these age and sex specific estimates to the population, CFAS I estimated that approximately 664,000 individuals aged 65+ in the UK would have dementia in 1991. CFAS II estimated that 670,000 people in the UK would meet the same study diagnostic criteria in 2011 (Matthews et al., 2013). Crucially however, the UK population had aged significantly in the two intervening decades, such that if the dementia prevalence rates within the 5-year age bands had remained consistent, 884,000 people would have been expected to have dementia in the UK in 2011 (Matthews et al., 2013). This 24% reduction equates to an estimated 214,000 individuals and their families not suffering the consequences of dementia in 2011.
The findings from these landmark studies, replicated in several other countries, showed us that some cases of dementia are preventable. When the population’s risk of dementia reduces in this way, for some this will mean dementia occurring later than it would have done, whilst for others they may never develop dementia before death. It is likely this population risk reduction is due to later generations enjoying healthier living conditions (such as better education, less exposure to tobacco smoke, healthier diets) and better medical care (of conditions like high blood pressure) across their lives than their parents.

Figure 30: CFAS I and CFAS II age-specific dementia prevalence. Image source: A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the Cognitive Function and Ageing Study I and II
What are the risk factors?
Prevention of any disease can focus on a) trying to interrupt the development of the disease process itself or b) by identifying and managing other conditions which put you at risk of developing the disease (‘risk factors’ – for example treating high blood pressure to in turn protect the brain’s blood supply and reduce dementia risk). Doing the former is theoretically attractive as it is very direct. But it has proven very difficult for dementia, probably because the biology of the disease process is complex and not sufficiently well understood. Also, because a person’s risk of dementia in old age (average age at onset in the CFAS studies was mid-80’s) represents a build-up of risk and protective factors accumulated right across their life – starting from their early years and educational opportunities, through to health behaviours in mid-life like healthy diet, alcohol, and smoking – all of which affects brain health.
Therefore, dementia risk reduction (or prevention) efforts often focus on trying to identify what the risk factors for developing dementia are and addressing these. The most comprehensive summary of evidence comes from the Lancet commission on dementia (Livingston et al., 2020). The Lancet commission determined that the evidence was convincing enough to consider 12 modifiable risk factors for dementia: less formal education in early life, midlife hearing loss, traumatic brain injury, hypertension, alcohol, and obesity, and late life smoking, depression, social isolation, physical inactivity, air pollution, and diabetes (Livingston et al., 2020). These factors typically affect dementia risk via changes to the brain tissue itself (e.g. head injuries), the building of ‘cognitive reserve’ so that function is maintained in spite of pathology (e.g. education), and/or through damage to the brain’s blood supply (e.g. hypertension).
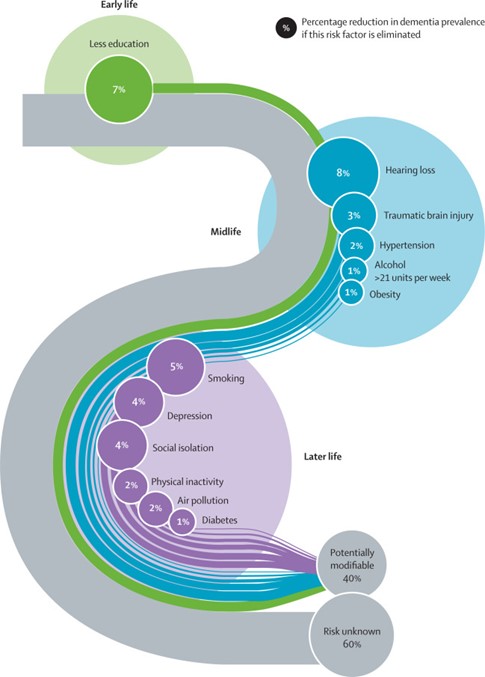
Figure 31: Life-course model showing the 12 potentially modifiable dementia risk factors. Image source: Dementia prevention, intervention, and care: 2020 report of the Lancet Commission
There are two important caveats to keep in mind:
- It’s not absolutely guaranteed that these 12 conditions cause someone to have an increased risk of dementia. Researching risk factors from across the life-course, for a disease that typically occurs at the end of life, is complex so we cannot conduct perfect studies. Equally, there are likely to be other risk factors, beyond these 12. But these 12 are the ones with the most convincing evidence of a causal link to dementia and it is at least likely that controlling these conditions will lower dementia risk. Further, each of these 12 risk factors are public health problems in their own right, so efforts to address them are warranted anyway, and a reduction in dementia risk can be seen as an added bonus.
- The evidence is usually collected at the group-level. This means that we cannot say to any single individual: ‘if you quit smoking you won’t get dementia, if you don’t you will’. Instead, we can say that if a whole population saw a drop in smoking rates, we would expect dementia rates to drop in future as a result (but not exactly which individuals would benefit).
Prevention strategies
We can think about addressing risk factors in different ways, and having a balance of each is important:
What can individuals do?
People (e.g. those who have parents living with dementia) often want to know what they can do to lower their own risk, and it is important that these people are given evidence-based and accessible information. For example, the NHS, Alzheimer’s Research UK and Alzheimer’s Society all have useful information for individuals. Related to this is work that can be done by partners across the system to raise awareness that dementia risk can be reduced, as some people are not aware of this and theoretically it could be a motivator for healthy behaviour change.
What can communities, populations and governments do?
Population-level strategies target the societal conditions that increase dementia risk (rather than encouraging individuals to lower their own risk in spite of these conditions). These interventions can operate at national (e.g. taxation of sugary drinks to reduce obesity, policies to address air pollution, improving access to education, mandating ear protection at noisy worksites) and local (e.g. restrictions of licences for fast food and alcohol establishments to reduce obesity and excess alcohol consumption) levels. These interventions have greater potential to reduce risk across the population and replicate the scales of reduction in prevalence seen in the CFAS data. They can also have equity effects because they typically make healthier choices easier or the default (or mandated), whereas individual-level interventions will typically be easier to achieve for those with more resources. A recent study pulled together and graded the quality of the available evidence on population-level interventions for dementia risk reduction (Walsh et al., 2024).
What can the NHS and other health services do?
The NHS has a role to play where there are evidence-based treatments for the risk factors of dementia. Conditions like hypertension, diabetes, depression, and hearing loss have established highly-effective treatments, and ensuring access to these along with high-quality care for these individuals can significantly reduce these risk factors (Livingston et al., 2020). For the very small number of people who develop reversible dementia, prompt diagnosis and treatment can make a significant difference to their long-term dementia outcomes.
Environmental factors
Social and environmental factors impact mental health across the life course. They are often ‘determined by structural factors which generate and perpetuate intergenerational cycles of disadvantage and poor health’ (Kirkbride et al., 2024). The evidence linking these factors to poor mental health is summarised in chapter one of this mental health needs assessment:
- Socioeconomic deprivation: The rate of income deprivation affecting older people is high in Peterborough and Fenland, with fewer deprived areas seen in other parts of Cambridgeshire (King & Leeman, 2019).
- Poverty and financial insecurity: National data shows 1 in 4 adults aged between 60 and 64 lived in poverty in 2022, the highest rate for any adult age group (Centre for Ageing Better, 2023b). 18% of pensioners live in relative poverty, with groups at greater risk including private tenants (37%) and people living in social housing (36%); Asian/Asian British (29%) and Black/Black British pensioners (25%); and single older women (26%) (Age UK, 2023).
- Housing, homelessness and environmental justice: National data shows that half of ‘non-decent’ homes (homes that fail to meet basic decency criteria as defined by the government) are headed by someone aged 55+; and 1 in 3 are headed by someone aged 65+ (Centre for Ageing Better, 2023b).
- Employment and working conditions: The proportion of older adults in who are economically active (in employment) ranges from 16.2% in Cambridge, to 9.8% in Fenland.
- Community wellbeing: Over 1 in 5 people in the UK aged between 65 and 74 volunteered at least at once a month in 2020/21(Tabassum & Fern, 2023).
Inequalities
Chapter Two of this mental health needs assessment highlights that groups more likely to experience poor mental health and inequalities in mental health services. However, there is limited research about the health inequalities faced by older people compared to other age groups (Haighton et al., 2019).
- Ethnicity: ethnic inequalities in health can accumulate over the life course and are ‘exacerbated in older ages’ (Stopforth et al., 2022). Research suggests that older people from ethnic minority backgrounds may face specific barriers in accessing health services due to digital exclusion and digital applications not being available in different languages (Kapadia et al., 2022).
- Sexuality: 43% of LGBT+ people aged 55+ are not confident that mental health services will understand and meet their needs, much higher than the rate than their heterosexual peers (Hudson-Sharp & Metcalf, 2016).
- Refugees and asylum seekers: One study suggests that there are high rates of PTSD, depression and anxiety amongst older adults who are refugees (C. J. Frost et al., 2019).
- Disability: Older adults with hearing loss are 2.5 times more likely to develop depression than those without hearing loss (J. Edwards et al., 2016).
- Carers: In 2022, the peak age group for providing care was 55- to 64-year-olds (Carers Week, 2022). The long-term caregiving of older carers is associated with a higher risk of depression (Steptoe et al., 2018).
- Homelessness: Peterborough had a significantly higher rate of households owed a prevention or relief duty under the Homeless Reduction Act in 2021/22 where the main applicant was aged 55+, compared to the national average.
- Offending: Older people in prison can age prematurely due to their living conditions and tend to have high rates of physical health problems (Durcan, 2020).
- Victims of crime: International research suggests that 15.7% of all adults aged 60+ have experienced some form of abuse in the past year (Yon et al., 2017). National data shows that 4.2% of women aged between 60 and 74, and 2.1% of men, have experienced domestic abuse in the past year (Office for National Statistics, 2023).
Physical health, polypharmacy and multimorbidity
What: Life expectancy is expected to increase over the next 20 years, whilst the age at which people develop major illnesses is predicted to remain constant (Watt et al., 2023). This means that there will be increasing numbers of older adults living with major illnesses and multiple long-term health conditions (multimorbidity); as well as those using multiple medications at the same time (polypharmacy). Multimorbidity has been called ‘one of the greatest challenges facing health services’ (Pearson-Stuttard et al., 2019). Each additional health condition means that people experience more symptoms, go through more treatments and are more likely to experience harmful effects from the interactions of medications (Centre for Mental Health & Age UK, 2024).
Who: National data shows that older multimorbidity increases with age, and that people living in more deprived areas are more likely to experience multimorbidity at a younger age.
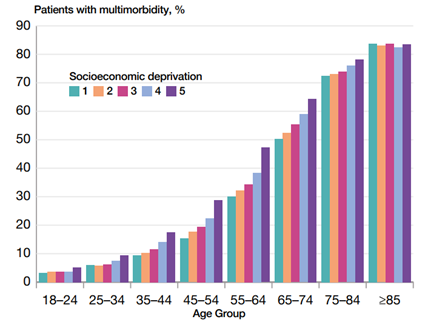
Figure 32: Prevalence of multimorbidity (2 or more conditions) by age and deprivation. Image source: Chief Medical Officer’s annual report 2023: health in an ageing society
Why is this important to mental health: Mental health conditions can make up all or part of multimorbidity. Many older adults with mental illness have physical health conditions, which is associated with lower quality of life, greater use of health care and linked to polypharmacy (Daunt et al., 2023). Physical ill-health is also strongly linked with mental ill-health: for example, the risk of developing depression is over 7 times higher in those with 2+ chronic physical problems (Naylor, Parsonage, McDaid, et al., 2012). The interaction of physical and mental health is described in more detail in chapter two of this mental health needs assessment.
One study found that around 2 in 3 of adults aged 70+ admitted to acute general hospitals in an emergency have co-existing mental health conditions (Goldberg et al., 2012). In a 500-bed general hospital, 330 beds will be occupied by older adults. This means that out of this group, 220 will have a mental health condition (Stickland & Gentry, 2016), with:
- 27% having been diagnosed with dementia.
- 27% experiencing delirium.
- 8% having definitive major depression, and a further 24% possible major depression.
- 50% having some form of cognitive impairment.
Older adults with co-existing mental and physical health problems have poorer outcomes (Public Health England, 2019b). Suboptimal care of older adults with multimorbidity is associated with longer stays in hospital and substantially higher healthcare costs. Earlier interventions by mental health providers (proactive care) can help people manage their mental health and are associated with lower healthcare costs (NHS England, 2018).
Frailty
What: Frailty is a ‘distinct health state related to the ageing process in which multiple body systems gradually lose their in-built reserves’ (Society, 2014), so individuals are less able to cope with and recover from illness and accidents. Frailty has a bigger impact on someone’s day-to-day life and their risk of being admitted to hospital than their age (Han et al., 2019). Frailty is not the same as physical ill-health or multi-morbidity: it is estimated that around three-quarters of people with frailty have multimorbidity, but that the majority of people with multimorbidity (85%) do not have frailty (Vetrano et al., 2019).
Who: Frailty prevalence increases with age: it is estimated 1 in 10 people aged 65+, and 1 in 4 people aged 85+, live with some form of frailty (Public Health England, 2019b). There was a greater increase in frailty with age over the period of austerity in England (Pugh et al., 2024).
Why is this important to mental health: Research suggests that there is a two-way relationship between depression and frailty, with one meta-analysis finding that 39% of people with frailty also experience depression and that psychological factors contribute to the development of, and outcomes from, frailty (Soysal et al., 2017). Frailty is also associated with an increased risk of delirium and dementia (Royal College of Psychiatrists, 2020). It is likely that people with older people with severe mental illness are at greater risk of frailty, although there is limited research in this area (Royal College of Psychiatrists, 2020).
Care homes
What: Care homes ‘provide accommodation and personal care for people who need extra support in their daily lives’ (Age UK, 2022a).
Who: In Cambridgeshire and Peterborough, 2 – 3% of people aged 65+ lived in care homes in 2021. This increases to 8 – 12% of people aged 85+. The proportion of older adults in care homes was highest in Cambridge City, and lowest in South Cambridgeshire, compared to other districts.

Figure 33: The proportion of usual residents aged 65+ and 85+ living in care homes, per total population in those age groups, Cambridgeshire and Peterborough, 2021. Data source: Census 2021. Note that data was collected during the early stages of the COVID-19 pandemic, in 2021, which may have impacted the number of residents in care homes.
The number of care home and nursing home beds in Cambridgeshire has remained relatively stable from 2011 to 2021, but there has been a 35% increase in the number of beds in Peterborough. The rate of permanent admissions to residential and nursing homes (per 100,000 of the older adult population) is below the national average in both areas.

Figure 34: Nursing and care home beds, Cambridgeshire and Peterborough, 2011 – 2021. Data source: Fingertips
Why is this important to mental health: The majority of people in care homes have a neurological condition (often dementia or stroke), with one estimate stating that 3 in 4 people in care homes have dementia (NHS England, 2017). Research suggests that around 8 in 10 people in this group have behavioural and psychological symptoms of dementia (Seitz et al., 2010). The prevalence of delirium amongst people receiving long-term care to be between 6 – 14% (Seitz et al., 2010). Between 40 – 80% people living in care homes experience depressive symptoms (Potter et al., 2018; Seitz et al., 2010) and 1 in 4 have clinical depression (Seitz et al., 2010). It is likely that depression is underdiagnosed in care home residents, with one study finding that fewer than a 1 in 4 cases were detected (Davison et al., 2007).
- Depression amongst care home residents is associated with functional decline, pain, loneliness and a greater mortality risk (Potter et al., 2018).
- Qualitive research with care home residents raises that loss of independence, loneliness, and aspects of living in a care home itself (such as staff turnover, lack of meaningful activities and lack of privacy) as causes of their depression (Choi et al., 2008)
- Many people with depression also experience some form of anxiety disorder. However, there is limited research on anxiety in care homes (Seitz et al., 2010).
NICE guidelines outline evidence-based approaches to support the wellbeing of older adults in care homes, including early assessment and access to appropriate mental healthcare (National Institute for Health and Care Excellence, 2013). However, in 2018 a survey found that 22% of care home managers in Cambridgeshire and Peterborough found it difficult to access mental health reviews and assessments (Cambridgeshire and Peterborough Older People’s Mental Health Delivery Board, 2018).
Loneliness and social isolation
What: Age UK defines loneliness as ‘a subjective feeling about the gap between a person’s desired levels of social contact and their actual level of social contact’ (Age UK, 2022b). This is different from social isolation, ‘an objective measure of the number of contacts people have’, which considers the quantity rather than quality of relationships. Different people may prefer to have different numbers of contacts, but loneliness is never desired (Age UK, 2022b).
Who: Loneliness can affect people of any age, but some older people may be particularly vulnerable. This includes people who are widowed, in poor health, live alone, do not feel they belong in their neighbourhood or are unable to do the things they want (Abrahams & Director, 2018). Surveys involving older adults highlight relationship breakdown and divorce as prominent negative experiences that have impacted their mood (Independent Age, 2020).
Research suggests that 7% of adults aged 50+ often feel lonely (Age UK, 2018a). Applying this figure to data from the 2021 Census, we estimate that there are 22,600 adults aged 50+ who are often lonely in Cambridgeshire and Peterborough. Another study involving adults aged 80+ in Cambridge City found that 25% felt ‘lonely’ and 16% felt ‘slightly lonely’ (Wang et al., 2019). Loneliness was more common among women, people with depression and people with high levels of physical impairment.
Why is this important to mental health: Connecting with other people is key for mental wellbeing. High levels of social engagement are associated with greater life satisfaction, physical health benefits and better cognition in older adults (J. Edwards et al., 2016), whilst the cumulative impact of loneliness is comparable to smoking in terms of health impacts (Holt-Lunstad et al., 2010); and is linked to a greater risk of developing dementia (Rafnsson et al., 2020) and depression (Zhang et al., 2023).
Additional resources
- The local data pack gives an overview of key data and trends
- WHO has developed guidelines on the integrated care for older people (ICOPE) which outline evidence-based recommendations to prevent, slow or reverse declines in the physical and mental capacity of older people.
- Older people: independence and mental wellbeing: covers the commissioning of services by local government and other local providers to help encourage and protect mental wellbeing and independence of older people.
- Dementia prevention: Population-Level Approaches to Dementia Risk Reduction (PLADRR) Research Group, Cambridgeshire & Peterborough All Age Dementia Strategic Plan 2018 – 2023, NICE guidance: dementia, disability and frailty in later life: mid-life approaches to delay or prevent onset
- Poverty: Briefing: Poverty in later life, Experiences of poverty in later life: mental health and wellbeing
- Carers: Caring into later life: The growing pressure on older carers, The Emotional Wellbeing of Older Carers
- Physical health conditions: Caring for the whole person: Physical healthcare of older adults with mental illness: Integration of care, Multiple long-term conditions (multimorbidity): making sense of the evidence
- Frailty: NICE guidelines for mid-life approaches to delay or prevent the onset of frailty, Proactive care: providing care and support for people living at home with moderate or severe frailty, Frailty: Ensuring the best outcomes for frail older people, End of Life Care in Frailty
- Care homes: NICE: mental wellbeing of older people in care homes, NICE: older people with social care needs and multiple long-term conditions, Depression among older people living in care homes. Providing proactive care for people living in care homes – Enhanced health in care homes framework, Promoting Emotional Health & Wellbeing and Preventing Suicide: A Resource for Care Home Settings
- Loneliness: Age UK loneliness research and resources, including All the Lonely People: Loneliness in Later Life; Promising approaches to reducing loneliness and isolation in later life; Royal College of Psychiatrists statement on loneliness and social isolation
References
Full list of references is included at the end of this chapter.