Homelessness
People experiencing homelessness face intersecting health and social issues, that require holistic interventions (Liu & Hwang, 2021).
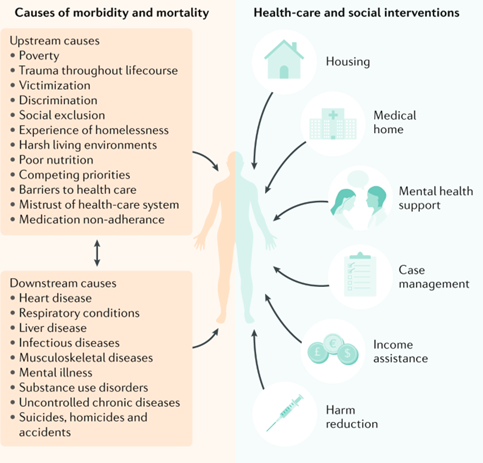
Figure 47: Homelessness, health, and healthcare and social interventions. Image source: Liu & Hwang 2021
Local population
The local picture on homelessness is covered in Chapter 1 of this report. The number of rough sleepers in Cambridge City was substantially higher in April, June and July 2022, than in previous years. A much higher proportion of men are recorded as sleeping rough than women. This number is likely to be an underestimate of true figures.
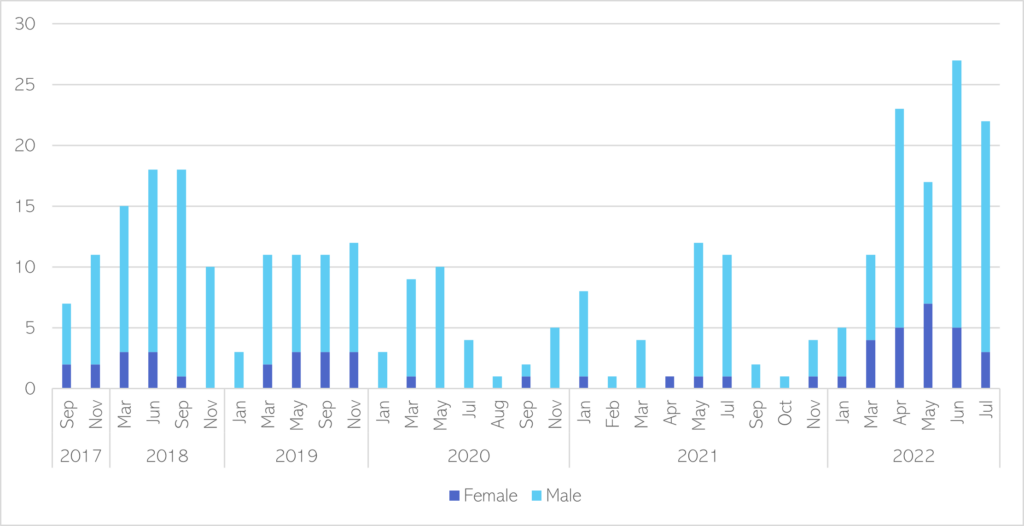
Figure 48: Verified number of rough sleepers in Cambridge City, Sep 2017 – July 2022. Data source: Inform dashboard for Cambridge City
Mental health need
- Mental illness can be a contributing factor to people becoming homeless (Local Government Association, 2017), as well as acting as a barrier which can prevent people from moving into stable accommodation (Tweed et al., 2022).
- Compared to the general population, people experiencing homelessness are (Public Health England, 2019b):
- 2 times more likely to have a common mental health condition.
- 5 times more likely to experience psychosis.
- 9 times more likely to die by suicide.
- One recent survey of people experiencing homelessness in the UK found that (Homeless Link, 2014):
- 1 in 5 had self-harmed.
- 1 in 3 had experienced suicidal thoughts.
- 18% had experienced hearing voices.
- In one survey of homelessness services, staff estimated that 2 in 3 clients showed characteristics consistent with personality disorders (Rees, 2009).
- Rates of mental health conditions are likely to be higher among people caught in the ‘revolving door’, between hostels, prison, hospitals and rough sleeping (Public Health England, 2019b).
- 82% of people who have slept rough in the past year have a mental health vulnerability (MHCLG, 2020).
- The majority of people in this group have multiple mental health conditions (MHCLG, 2020).
- One survey of people accessing homelessness services found that (Evolve Housing + Support, 2018):
- Almost 4 in 5 (79%) had experienced at a traumatic event before the age of 18, of whom two thirds had experienced 3+ traumatic events.
- 29% felt that their experiences of childhood trauma were the main cause of their homelessness.
Co-occurring needs
The majority of people experiencing homelessness are likely to have other needs which impact their mental health, such as substance use, poor physical health, and traumatic brain injury.
- There are high rates of mental health conditions, physical ill health and disability, and experiences of domestic abuse amongst households owed a prevention or relief duty in Cambridgeshire and Peterborough (DLUHC, 2022a).
- The proportion of households in Fenland who have additional support needs is substantially higher than the national rates for most of types of support needs.
- The proportion of households with a history of mental health problems is higher than the national average in all Cambridgeshire districts, whereas it is lower in Peterborough.
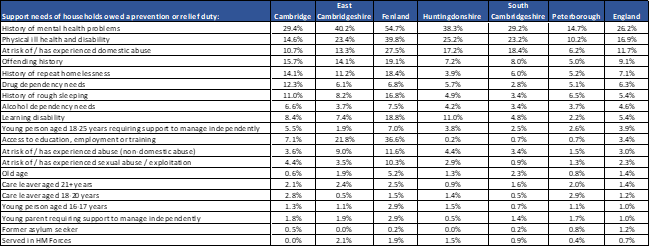
Figure 49: Support needs of households owed a homelessness duty in C & P, 2021 – 22. Data source: (DLUHC, 2022a)
- A review of people accessing housing-related support services in Cambridgeshire and Peterborough in 2017 identified that the majority of people were identified as having multiple needs: 58% had 3+ recorded support needs, and 18% had 5 support needs (the maximum number that could be recorded) (Commissioning Review of Homelessness, 2018).
- There are likely to be high levels of co-occurring substance use and mental health conditions amongst people experiencing homelessness. This group have more severe physical and psychological symptoms than other people experiencing homelessness (Schütz et al., 2019).
- Exact figures vary significantly depending on how homelessness, substance use and mental health conditions are defined. The stigma around these issues prevents many people from seeking help or having their needs recorded, as a result many figures are likely to be underestimates. For example, one recent survey of people experiencing homelessness found that almost half had used alcohol and/or drugs to cope with mental health issues (Homeless Link, 2014).
- People who are sleeping rough, living in squats or sofa surfing are more vulnerable to drug and alcohol use than those living in supported accommodation (Homeless Link, 2014).
- Mental health needs of people who are rough sleeping almost always co-occur with other vulnerabilities, including physical health needs, drug use and contact with the criminal justice system (MHCLG, 2020).
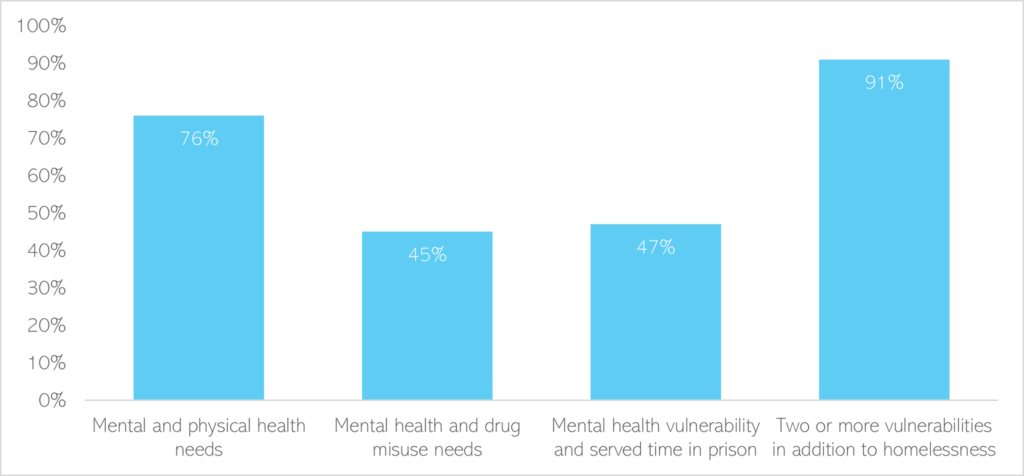
Figure 50: Support needs of people who have slept rough within the last year. Data source: (MHCLG, 2020)
- People experiencing homelessness are more likely to have had a traumatic brain injury (TBI), which can impact mental health and behaviour; and can contribute to people being perceived as ‘hard to reach’ and being excluded from services (Everitt & Kaur, 2019):
- It has been estimated at 43-53% of people experiencing homelessness have had a TBI.
- People experiencing homelessness are 5 times more likely to have been hospitalised following a brain injury, compared to the general population.
- There is some evidence to suggest that autistic people are more likely to experience homelessness (Churchard et al., 2019). One small survey of people with long-term experiences of homeless found that (Churchard et al., 2019):
- 12% met autism criteria,
- 9% had elevated autistic traits,
- Yet only 1% had a pre-existing autism diagnosis.
Subgroups of people experiencing homelessness
There is limited research into the specific mental health needs of subgroups of people experiencing homelessness, such as LGBTQ+ people (Rees, 2009). However some research does highlight that specific groups have different needs.
Women
- Women often become homeless after prologued traumatic experiences, including emotional and sexual domestic abuse. A survey of people accessing support from one homelessness service found that (St Mungo’s, 2014):
- 70% had mental health needs.
- 27% had a combination of mental health, physical health and substance use needs.
- 50% of the women they supported had experienced domestic abuse and 19% had experienced abuse as a child; compared to 5% and 8% of men.
- Almost half of the women they supported had children, the majority of whom (79%) had children taken into care or adopted.
- Another recent survey of women experiencing homelessness found that (Groundswell, 2020):
- Almost 2 in 3 (64%) had mental health conditions, most commonly depression (45%), anxiety disorders (29%) and PTSD (18%).
- Substance use was highlighted as both a cause and consequence of homelessness, with a quarter (24%) of participants feeling that addiction was affecting their day-to-day life.
- Almost 3 in 4 had physical health conditions which had been exacerbated by their living situation.
- 39% had experienced domestic abuse.
- 1 in 4 had experienced sexual abuse.
- A study of women accessing homelessness support services found that (Evolve Housing + Support, 2018):
- 86% had experienced childhood trauma (a traumatic event before the age of 18), most commonly emotional abuse, family breakdown and separation, and violence within their family.
- 82% of women had experienced traumatic events since becoming homeless, most commonly emotional abuse, family breakdown and grief.
Children and young people
- The estimated prevalence of mental health conditions in young people experiencing homelessness ranges from 48 to 98% (Hodgson et al., 2013).
- A national survey of parents living in temporary accommodation found that (Shelter, 2022):
- 1 in 4 (26%) felt their child was often depressed or unhappy due to their living situation.
- 1 in 3 reported their child or children had to share a bed with siblings or other family members.
- 45% reported that their child or children had arrived at school late, tired or hungry due to their living situation.
- Compared to their peers, children and young people experiencing homelessness have (Gultekin et al., 2020):
- Poorer mental health, with longer periods of homelessness being associated with a greater incidence of mental health conditions and more severe symptoms.
- Poorer physical health, with one finding that 70% of 9- to 11-year-olds experiencing homelessness had at least one chronic health condition.
- There is a strong link between poor mental health, substance use and victimisation in unaccompanied and runaway youth who become homeless (Gultekin et al., 2020).
Migrants
- People experiencing homelessness who are not originally from the UK may face additional challenges, including restricted entitlements to support due to their immigration status (Boobis et al., 2019).
- Migrants can be highly vulnerable to exploitation when they are unable to access benefits and have precarious housing (Boobis et al., 2019).
Ethnic minorities
Black people are 3.5 time more likely to experience statutory homelessness as White British people (Bramley & Glen, 2022). The factors that contribute to these inequalities include demographics (such as age), discrimination, employment, local housing markets and poverty.
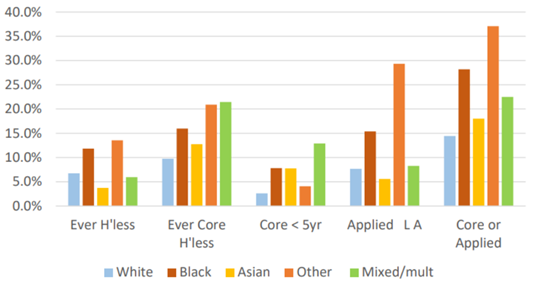
Figure 51: Percentage of adults meeting different measures of homelessness by broad ethnic groups in the UK, 2020. Source: (185). Note: this graph shows the percentage of people who: have ever been homeless, who have ever been core homeless (this refers to the most extreme and immediate forms of homelessness, such as rough sleeping, sofa surfing and staying in hostel accommodation), have been core homeless within the last year, those who have applied to a local authority and found to be homeless or at risk of becoming homeless in the next 56 days, and those who ever been experienced core homelessness or applied to a local authority and found to be homeless.
Access
A detailed report has recently been written by CHIRN (Cambridge Homelessness Impact Research Network) on Mapping healthcare barriers for people experiencing homelessness in Cambridge.
- Only 45% of rough sleepers with a mental health vulnerability and 61% of those with a drug use need received any form of treatment within the last year (MHCLG, 2020).
- Over recent years, there have been improvements in the rates of people experiencing homelessness who are registered with GPs (Homeless Link, 2014). However, there are still high levels of people accessing support in crisis, with one recent survey of people experiencing homelessness finding that within the past 6 months (Homeless Link, 2014):
- 82% had at least one GP appointment.
- 41% had visited accident and emergency services.
- The switch to telemedicine as a result of the COVID-19 pandemic (Lenhard et al., 2022):
- Made it more likely that some people experiencing homelessness attended their appointments and helped to provide continuity of care during lockdown restrictions.
- Some groups were less likely to benefit, such as women, older people, and those with less experience of technology.
- The use of telemedicine also raised issues of privacy and access to reliable technology.
Summary: ‘Knowing where to turn’: access to mental health support whilst experiencing homelessness (Groundswell, 2022b)
This report based on interviews with people experiencing homelessness highlights that people face a range of barriers to accessing mental health support. These include:
- That a lack of suitable accommodation exacerbates mental health issues and means that people are unable to prioritise accessing mental health support.
- People experiencing homelessness face additional stigma around mental health conditions, which can make it difficult for them to seek help. This stigma can be perpetuated by healthcare professionals, particularly for people with co-occurring mental health and substance use issues.
- People often lack trust in mental health services and professionals, and many do not know where to go to access mental health support. Many people needed support from a case worker or support worker to navigate the complexities of support systems.
- Some people reported that the first time they were able to access support was after their mental health had got significantly worse or when they were in crisis.
- When people were in contact with the mental health system, transitions between services and areas meant they often had to re-tell their story, re-refer themselves into services or even completely restart the process of accessing help.
People experiencing homelessness often find it difficult to access health services, including mental health care (Public Health England, 2019b). Barriers include:
Structural barriers to accessing mental health support:
- A lack of coordination between mental health services and other support services (Pleace & Bretherton, 2020).
- Healthcare professionals are not always provided with adequate resources to meet the needs of people experiencing homelessness (Siersbaek et al., 2021).
- Short and unreliable funding cycles can mean that staff perceive their employment as unstable, resulting in difficulties hiring and retaining experienced staff (Siersbaek et al., 2021).
Healthcare system barriers to accessing mental health support:
- Overly complex referral pathways into mental health services [(Pleace & Bretherton, 2020)(Groundswell, 2022a)].
- People being placed on long waiting lists [(Pleace & Bretherton, 2020)(Groundswell, 2022a)].
- Difficulties re-entering mental health services, which is demonstrated by one person’s experience of being on a ‘waiting for about five years now … because I go to prison …. I go to the bottom of the list and then it’s like restart’ (Groundswell, 2022a).
- A lack of 24-hour mental health support, which is particularly difficult for people who need help late at night (Groundswell, 2022a).
- A lack of accessible mental health support, except for during times of crisis (Pleace & Bretherton, 2020).
- Some healthcare staff lack expertise in the needs of people experiencing homelessness (Siersbaek et al., 2021).
- People with experiences of homelessness report having faced stigma and shame when interacting with healthcare services, particularly around past or current substance use, leading some people to avoid healthcare (Purkey & MacKenzie, 2019).
Individual barriers to accessing mental health support:
- Past negative experiences of services can lead people to delay seeking help until they have acute needs (Siersbaek et al., 2021).
- People with co-occurring substance use and mental health conditions experience additional barriers to accessing healthcare, which are explored more in the section on severe multiple disadvantage.
-
Experience
- A survey of 700 people experiencing homelessness people across England found high levels of unmet need in relation to mental health, and drug and alcohol use (Homeless Link, 2014):
- 41% had unmet alcohol use needs.
- 25% had unmet drug use needs.
- 46% had unmet mental health needs.
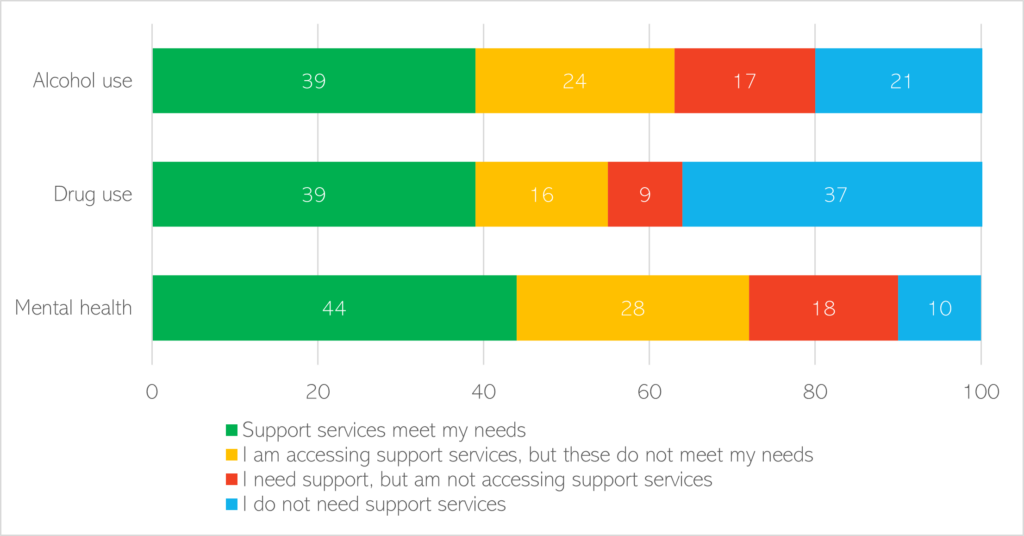
Figure 52: The percentage of unmet need relating to alcohol use, drug use and mental health in people experiencing homelessness. Data source: (Homeless Link, 2014)
- People experiencing homelessness report that healthcare systems are often not accountable to people experiencing homelessness and fail to take into account their specific needs(Purkey & MacKenzie, 2019). Examples included a lack of openness to harm reduction approaches to substance use, or a lack of flexibility for people who miss appointments.
- A recent survey of women experiencing homeless found that only 45% felt that healthcare services understood the specific issues they faced (Groundswell, 2020).
- A 2020 review into housing support services in Cambridgeshire and Peterborough highlighted there is a need for (Commissioning Review of Homelessness, 2018):
- More early intervention and easier access to mental health support, as well as more ongoing low-level mental health support
- Greater support for people with ‘complex needs’, including reducing the barriers that people with substance use face when accessing appropriate supported accommodation and community support; and additional support for people with enduring mental health conditions and those who have experienced domestic abuse.
Outcomes
- Overall health outcomes for people experiencing homelessness in England are extremely poor: they are significantly more likely to die from preventable and treatable causes; and the average life expectancy for this group is just 47 years (Perry & Craig, 2015).
- It has been estimated that 12 people experiencing homelessness died across Cambridgeshire and Peterborough in 2021, the second highest number in the past 8 years (Office for National Statistics, 2022a).
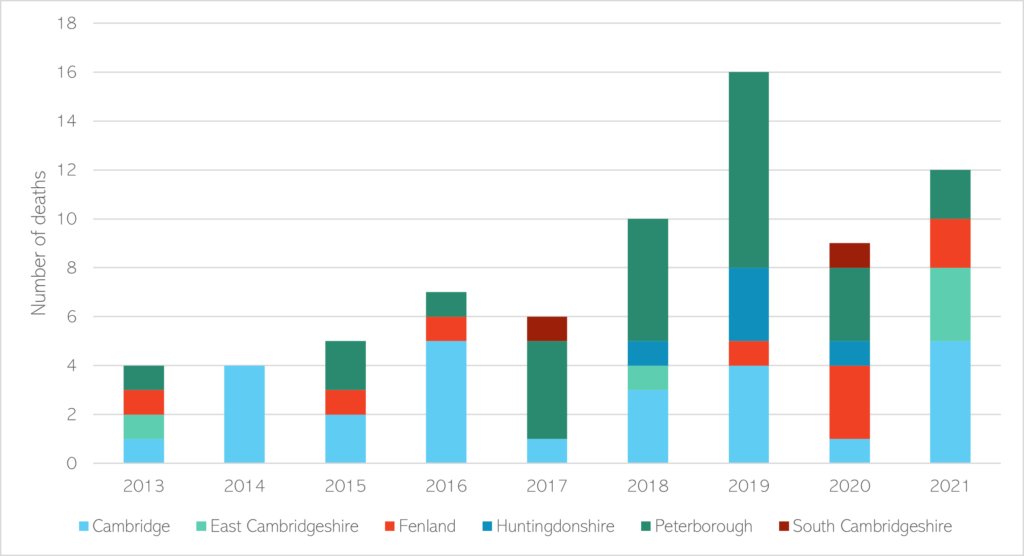
Figure 53: Estimated number of deaths amongst people experiencing homelessness across Cambridgeshire and Peterborough, from 2013 to 2021. Note that these figures are conservative estimates and real numbers may be higher. Data source: (Office for National Statistics, 2022a).
Additional resources
- The local data pack gives an overview of key data and trends
- NICE guidelines on Integrated health and social care for people experiencing homelessness
- Homeless Link’s report The Unhealthy State of Homelessness: Health Audit Results 2014
- Groundswell’s reports #HealthNow Literature Review Update: How has patient experience changes for people who are homeless? and ‘Knowing where to turn’: access to mental health support whilst experiencing homelessness
- Shelter’s report Growing up Homeless
- Homelessness and mental health resources
References
Full list of references is included at the end of this chapter.