Severe multiple disadvantage
Severe multiple disadvantage (SMD) is a term used to describe people experiencing a combination of (Harland et al., 2022): mental ill health, homelessness, substance use, domestic abuse, and/or offending. This is sometimes referred to as ‘multiple complex needs’ and ‘multiple exclusion homelessness’ (Harland et al., 2022).
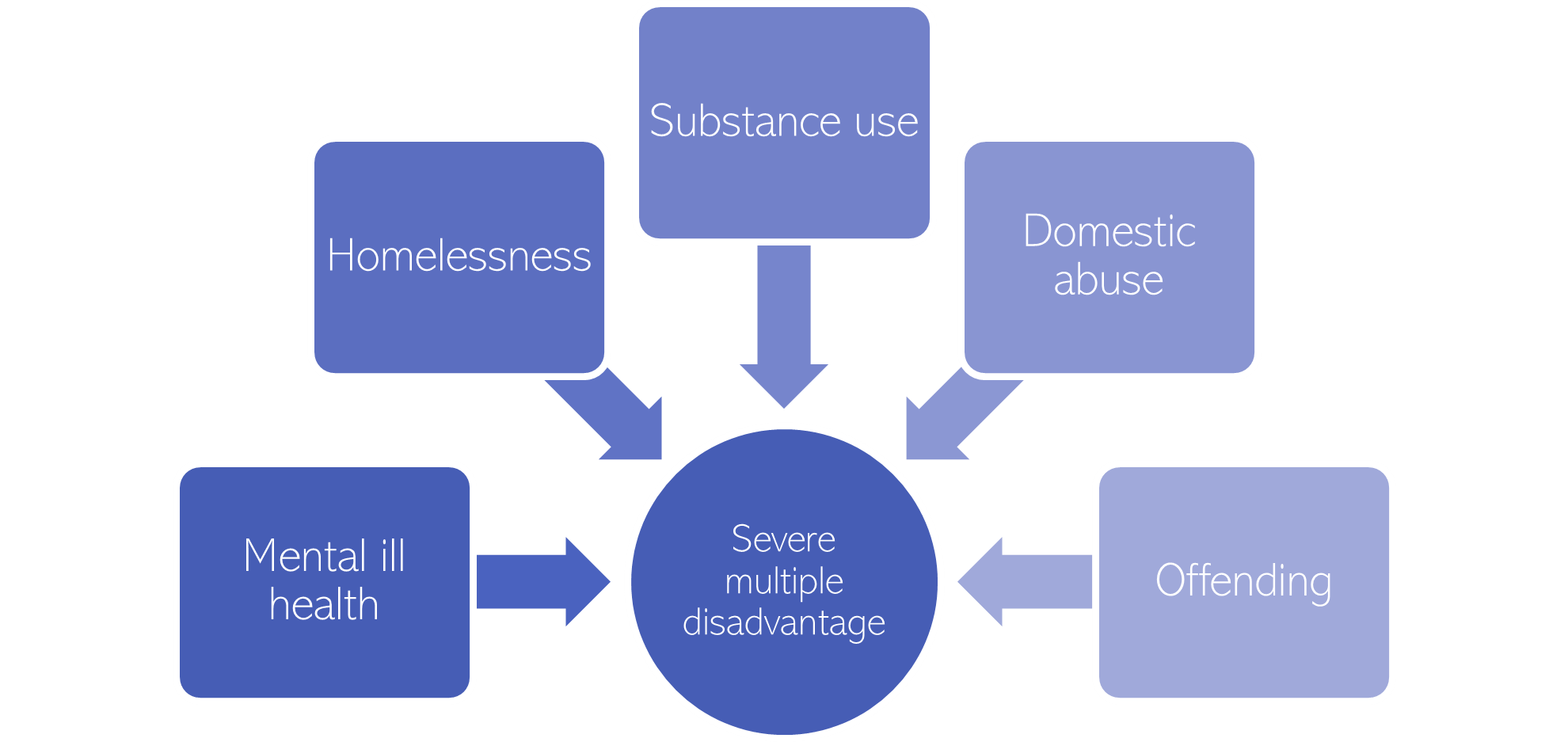
Figure 54: The five aspects of severe multiple disadvantage
Some have argued that this definition should be expanded to include:
- The total prevalence of SMD over the life-course, rather than focusing solely on those experiencing multiple disadvantages simultaneously or within a short timeframe, as these experiences can have substantial cumulative impacts on individuals (Sosenko et al., 2020).
- Neurodivergence as another aspect of SMD, as people can be disadvantaged because of a lack of support around neurodivergence. Examples include (Revolving Doors, 2022):
- Substance use to ‘mask’ neurodivergent behaviours.
- The behaviour of neurodivergent people is often misinterpreted, potentially making them more likely to be arrested.
- Neurodiverse conditions often go unrecognised and/or are not always considered as part of mitigating circumstances within the criminal justice system.
Local population
It is estimated that around 1,300 people across Cambridgeshire and Peterborough experience at least two of: homelessness, contact with the criminal justice system, and substance use (Hill, 2021; Office for National Statistics, 2022c). These figures are likely to be underestimates, particularly in terms of the number of women experiencing SMD (Bramley et al., 2015). Furthermore, whilst this estimate is based on the most comprehensive national estimate of SMD currently available, it was made in 2015.
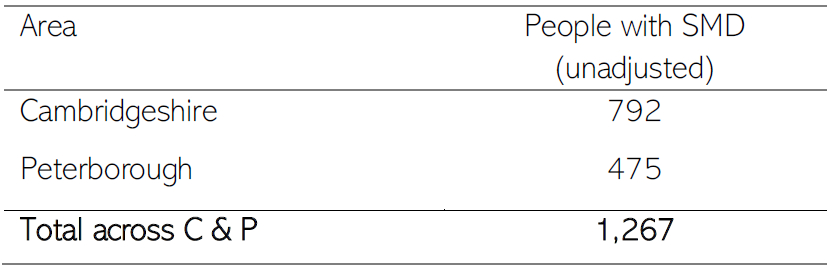
Figure 55: Estimated number of people experiencing SMD, based on the proportions of SMD estimated in the Hard Edges report (1.8 people per 1,000 working-age population in Cambridgeshire and 3.4 per 1,000 in Peterborough face SMD) and 2022 population estimates of 15 – 64 year olds. Data sources: (Hill, 2021; Office for National Statistics, 2022c)
- The proportion of people in alcohol treatment with an urgent housing problem is 2 times the national rate in Cambridgeshire, and 4 times the national rate in Peterborough.
- The proportion of people in alcohol treatment identified as having a housing problem is over twice the national rate (7%) in Peterborough (15%).
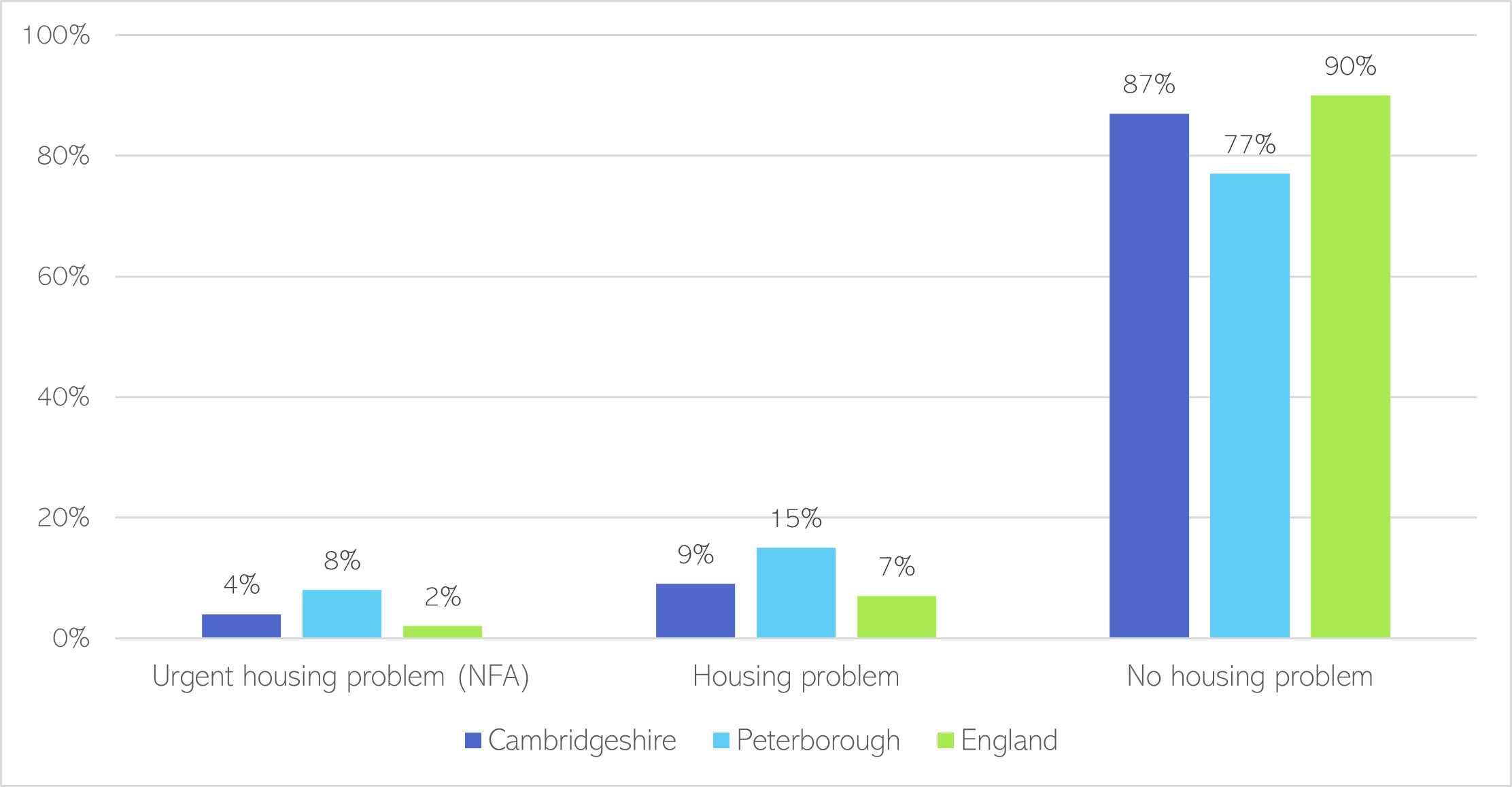
Figure 56: Accommodation status of new presentations of adults in alcohol treatment at the start of treatment, 2020-21. Note that NFA refers to people with no fixed abode; and that 1% of national data is missing, so these figures do not add up to 100%. Data source: NDTMS
- Changing Futures works to improve outcomes for people with SMD in Cambridgeshire and Peterborough.
- The following data summarises people who met criteria for SMD and were accepted for support between 2011 and mid-January 2023. As such it does not give a representative picture of overall local levels of SMD.
- To meet the criteria for this programme, people must be identified as having at least 3 of the following needs: homelessness, diagnosed or underlying mental health condition, alcohol use, substance use, domestic abuse or other forms of abuse, contact with the criminal justice system or time spent in prison, and physical health issues.
- People accessing Changing Futures often face homelessness, substance use and contact with the criminal justice system. Around half have been diagnosed with a mental health condition.
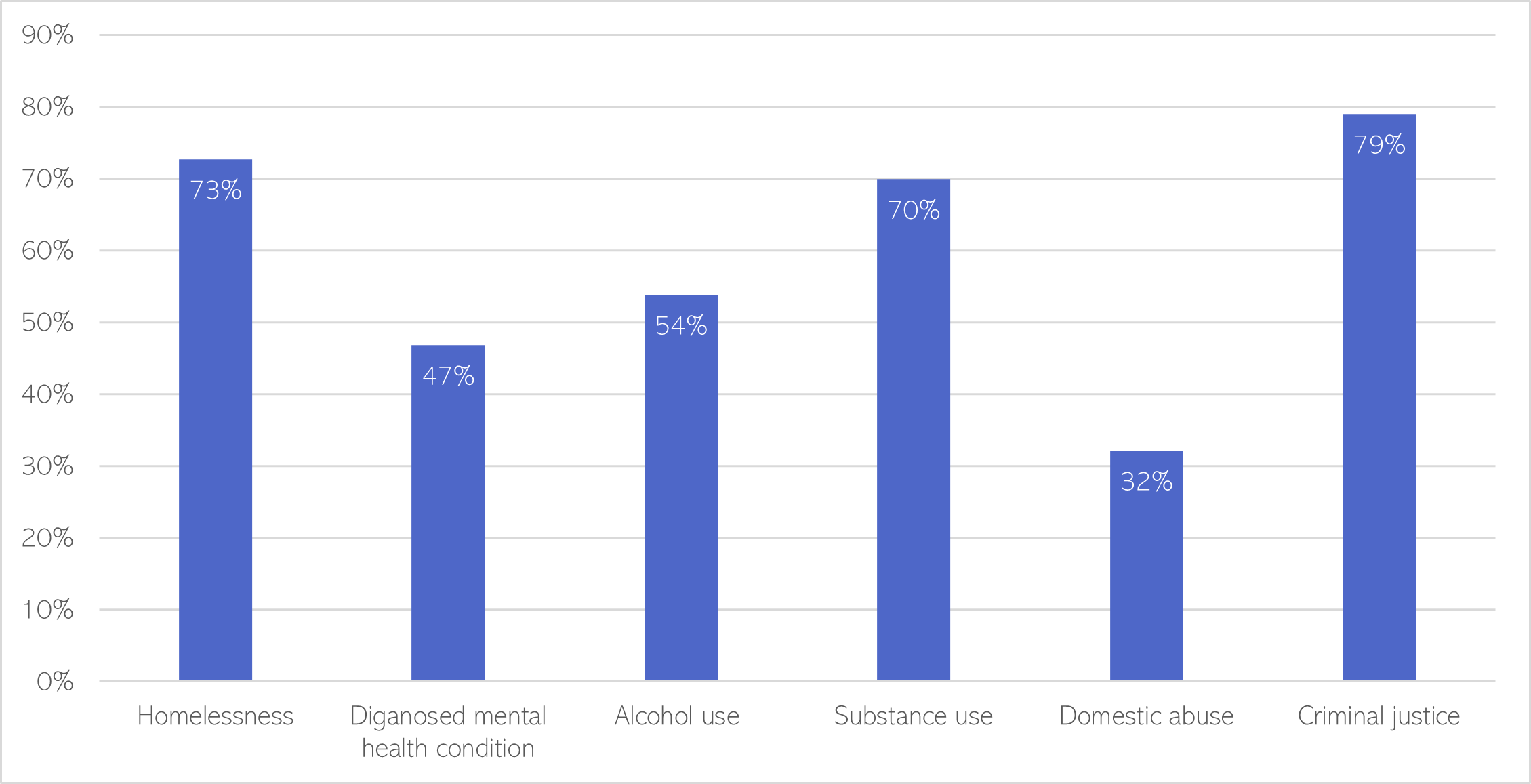
Figure 57: Needs of the Changing Futures cohort, from 2011 to mid-January 2023.
- A substantial proportion of the Changing Future cohort experiences a combination of homelessness, substance use and contact with the criminal justice system.
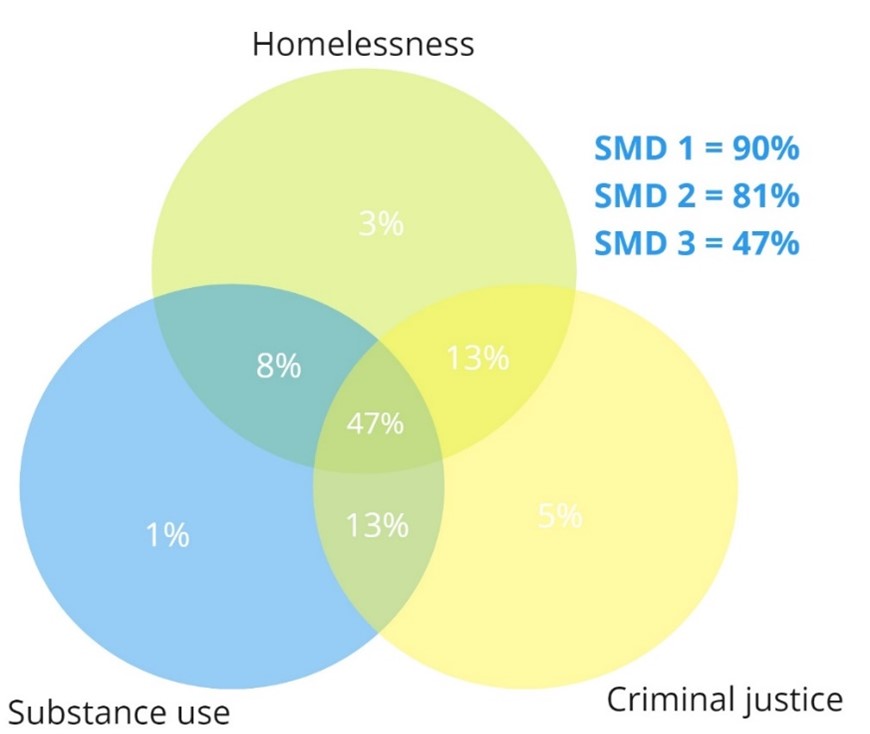
Figure 58: Overlapping experiences of SMD within the Changing Futures cohort, shown as percentages of the overall cohort (rounded to the nearest percent).
- The majority of people supported by Changing Futures are between 35 and 50 years of age (38%) or aged between 25 and 35 (29%).
- The majority of referrals into the Changing Futures programme are from Cambridge City and Peterborough.
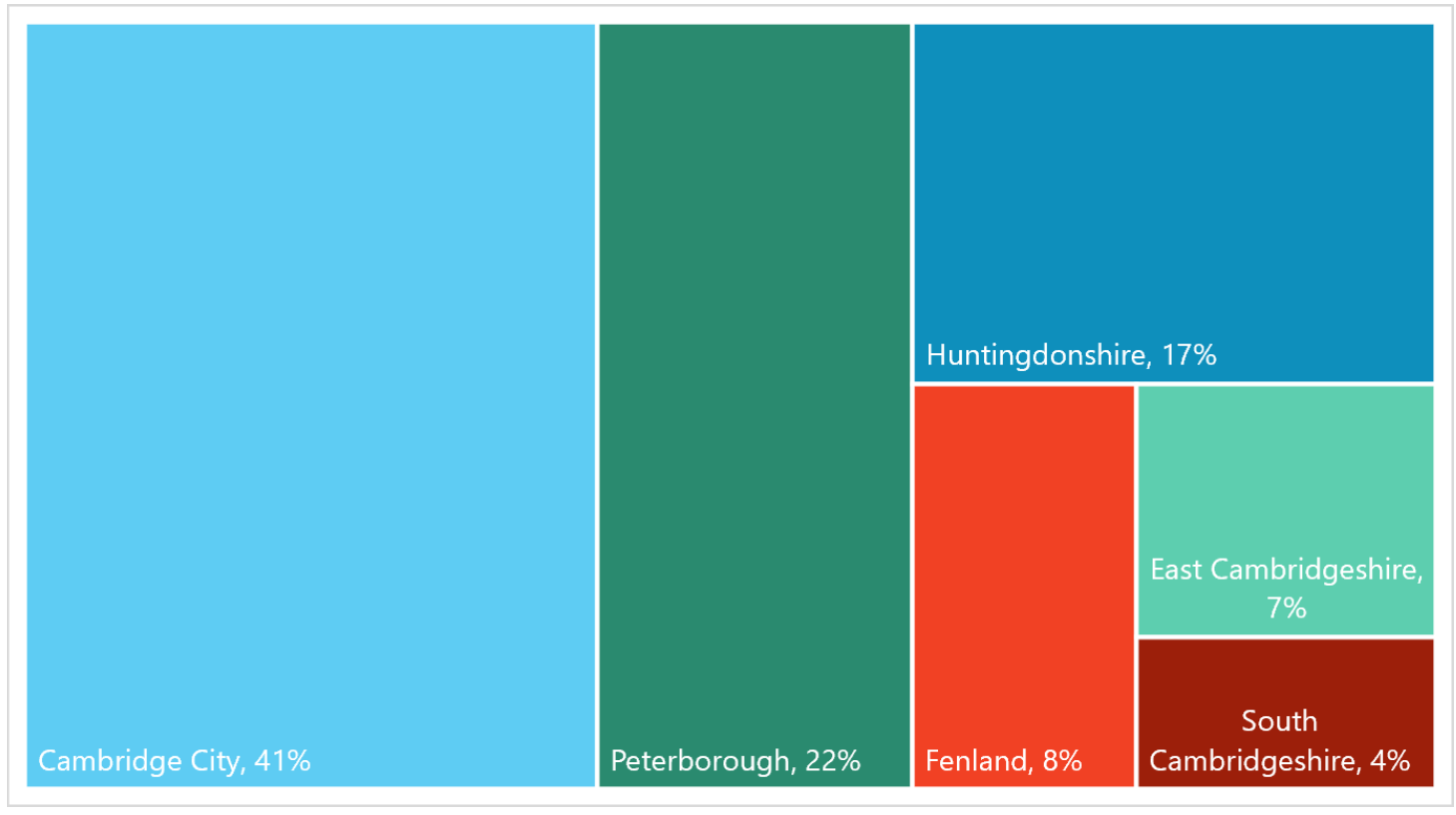
Figure 59: Percentage of accepted referrals to the Changing Future programme, by district.
Who is impacted by SMD?
- People impacted by a combination of substance use, offending, and homelessness are predominantly white men aged between 25 and 44 (Bramley et al., 2015).
- However, there is also a ‘hidden need’ amongst people from ethnic minority groups, particularly amongst Asian people, who may be less likely to fit this definition of SMD or to engage with mainstream support services (Everitt & Kaur, 2019).
- When domestic abuse is included as part of SMD, then the balance between men and women experiencing SMD is approximately equal (Everitt & Kaur, 2019).
- It has been estimated that almost 60% of people with experiences of homelessness, contact with the criminal justice system and mental health conditions either live with or have ongoing contact with their children (Bramley et al., 2015). This highlights the wider social impact of SMD.
Summary: Women and SMD
- 1 in 20 women have experienced extensive physical and sexual violence, compared to 1 in 100 men (Scott et al., 2015).
- There are close links between domestic abuse, poor mental health and substance use (Robinson, 2016). Domestic abuse is also a leading cause of homelessness (Robinson, 2016); and the majority of women in prison have faced domestic or sexual violence (Agenda, 2019).
- The ‘Hard Edges’ report, one of the most detailed quantitative studies of people with SMD, found that only around 22% of people affected by homelessness, offending and substance use are women (Bramley et al., 2015).
- However, women experiencing homelessness may be missed by researchers. They often reduce their visibility when rough sleeping as they are often very conscious of their own vulnerability. They are also more likely to end up ‘sofa surfing’ rather than live in hostels (Robinson, 2016).
- There are higher rates of mental health conditions amongst women experiencing homelessness, than men (Robinson, 2016).
- A 2017 report found that, out of 173 local areas in England and Wales, only 19 provided support for women which could address all of the following issues: mental health conditions, substance use, offending and homelessness (Agenda, 2019).
What proportion of people experiencing homelessness have experiences of SMD?
There is thought to be a high prevalence of SMD within people experiencing homelessness, although prevalence varies across surveys, due to small sample sizes and differences in definitions of substance use and mental health.
- One survey found that 92% of people experiencing homelessness, offending and substance use have a self-reported mental health problem (Fitzpatrick et al., 2011).
- Another survey of people using homelessness services found that 2 in 3 people were either in drug treatment or had contact with the criminal justice system (Bramley et al., 2015).
- One survey of people with experiences of homelessness, and at least one of: substance use, institutional care (such as time spent in prison or in the care of a local authority), or ‘street culture’ activities (such as begging) found that (Fitzpatrick et al., 2011):
- 63% had a period in their life when they had 6+ alcoholic drinks each day.
- 46% had spent time in prison.
- 29% had spent time as an inpatient in a mental health unit.
- A survey of people who had experienced homelessness and substance use found high rates of anxiety and/or depression (95%), and that a large proportion of people had spent time in prison (77%) (Fitzpatrick et al., 2011). Almost all the women who took part in this survey had experiences of ‘survival sex work’ (Fitzpatrick et al., 2011).
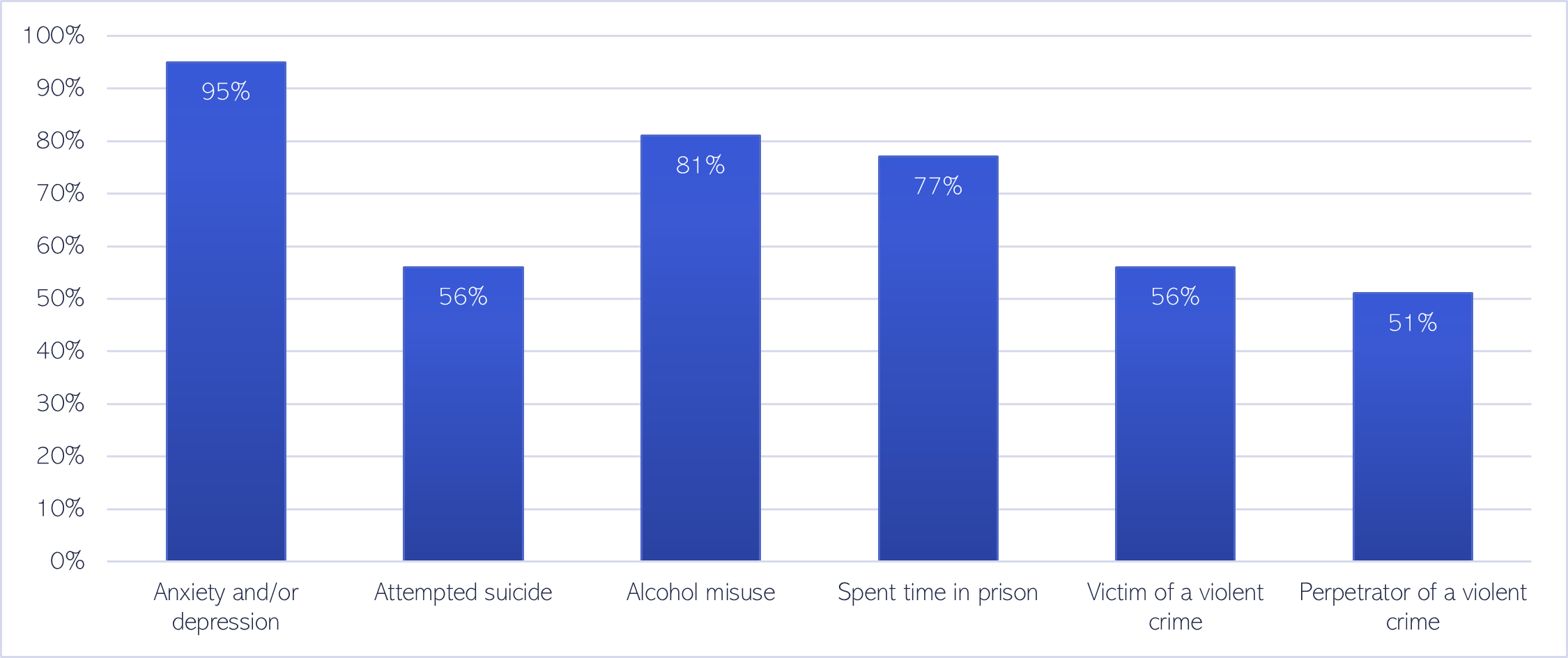
Figure 60: Percentage of people with experiences of homelessness and substance use, who also had the following experiences. Data source: (Fitzpatrick et al., 2011)
Another survey found that 60% of people who were rough sleeping had a substance use need (MHCLG, 2020):
- 49% had a drug support need.
- 23% had an alcohol support need.
- 12% had both a drug and alcohol support need.
What proportion of people who have experienced domestic abuse experience SMD?
- There are strong links between domestic abuse and homelessness: 1 in 11 households in England who were homeless or threatened with homelessness in 2019/20 recorded domestic abuse as the main reason (Office for National Statistics, 2021b).
- One survey of women seeking support for rough sleeping found that 35% had left home to escape violence (Office for National Statistics, 2021b).
Mental health need
SMD issues are ‘progressive, rooted in childhood and linked to underlying social and structural factors, outside of the control of the individual, and many the result of social exclusion’ (Harland et al., 2022).
- Multiple adverse childhood experiences, including abuse, being in care and parental imprisonment, are common amongst people with experiences of SMD [(191)(197)]. One study found that approximately 85% of people with experiences of SMD have had significant childhood trauma (29).
- The early life of people with experiences of SMD often included:
- Poverty (29),
- Difficult or unhealthy family relationships (29).
- Very poor experiences in the education system (29).
- People experiencing SMD report (191):
- That poor mental health often preceded their experiences of SMD, particularly if co-occurring substance use issues prevented them from accessing mental health support.
- Early experiences of homelessness and unstable housing were major contributors to their adult experience of SMD.
- One survey of people experiencing SMD in the form of homelessness and poor mental health found that (198):
- 48% had been in local authority care as a child.
- 71% had been a victim of a violent crime.
- 40% had been sexually assaulted as an adult.
- 61% had spent time in prison.
- There are also high levels of poor physical health amongst people facing SMD: one programme supporting people experiencing SMD found that 42% of people had a disability or long-term limiting condition (31).
- Women with experiences of SMD report experiencing disadvantage relating to the following factors, many of which are linked to discrimination and social exclusion (192):
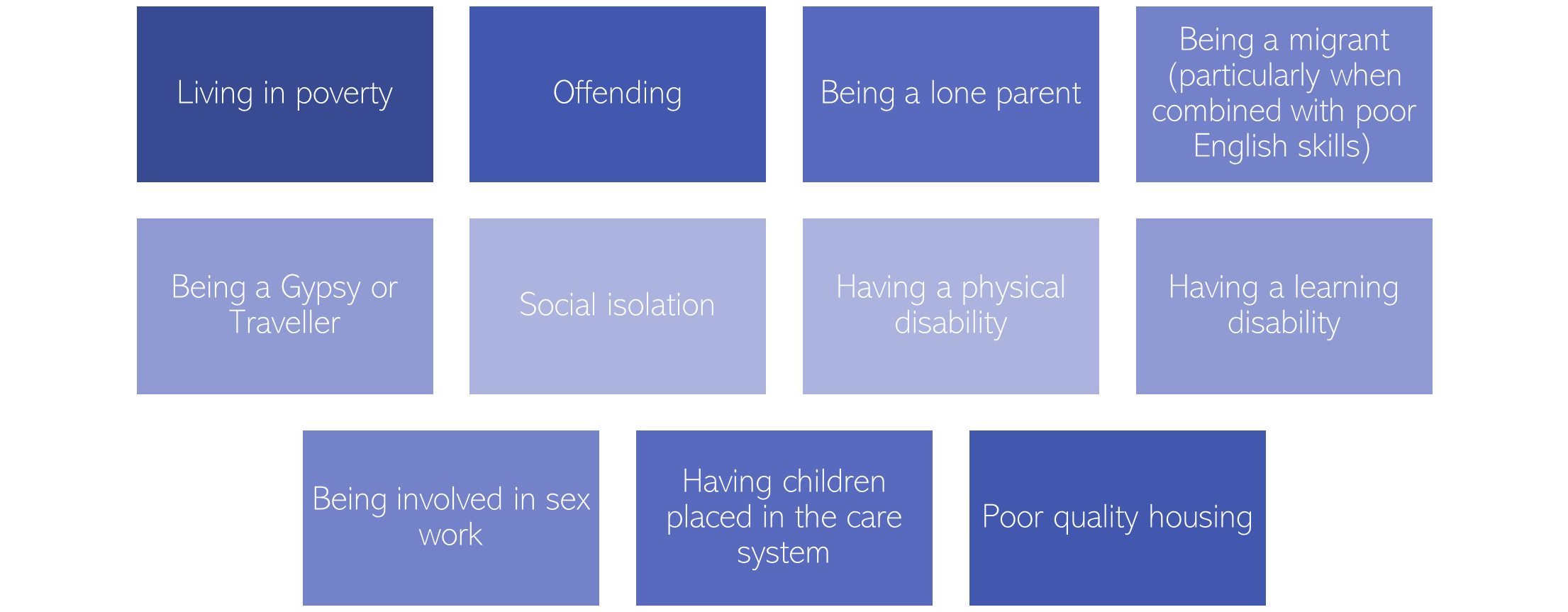
Figure 61: Factors identified a ‘secondary domains of disadvantage’ by women with experience of SMD. Adapted from: (192)
- People involved in street-based sex work are likely to have overlapping experiences with SMD. One review of services for street-based sex workers in a London borough found that (199):
- 86% of women supported by local services used crack cocaine.
- 37% of women supported by local services drunk alcohol every day.
- A quarter reported having mental health problems, although there was evidence to suggest that a higher proportion had undiagnosed or unrecognised mental health conditions, including PTSD, personality disorders, anxiety and depression.
- Stigma was a significant barrier preventing people from accessing support services.
- Community-level risk factors for SMD include (29):
- Demographic factors: a high proportion of the population being aged between 16 and 24 and/or large numbers of single person households.
- Economic factors: high rates of poverty and/or unemployment.
- Housing factors: a high proportion of smaller properties in the local housing market.
- Health factors: poor overall health of the population.
- Institutional factors: large institutional populations, including people living in homeless hostels or as inpatients on mental health wards.
Access
‘Our support system treats people based on what it considers to be their primary need, be that mental ill-health, dependence on drugs and alcohol, homelessness or offending’ (200)
People with experiences of SMD report (Harland et al., 2022):
- Early intervention provided in their late teens or early twenties may have been critical in preventing their experiences of SMD, particularly mental health support.
- Improved access to mental health, housing, and welfare services would have prevented their circumstances from worsening, especially the provision of non-judgmental support.
Barriers to accessing mental health services faced by people experiencing SMD:
Structural barriers to accessing mental health support
- A lack of coordination between mental health, substance use, housing and criminal justice services. This lack of coordination occurs at all levels, from frontline staffing to commissioning and strategies (Everitt & Kaur, 2019).
- Some people experiencing homelessness report not being able to focus on recovery from substance use or mental health conditions because they need to prioritise other issues such as housing (Adams, 2022).
- People from ethnic minority backgrounds with experiences of SMD report being unable to access services due to poverty, which is a particular problem for people who have no recourse to public funds (Robinson et al., 2017).
Healthcare system barriers to accessing mental health support
- Mental health systems and referral pathways can be difficult to navigate for people with multiple needs, both for people experiencing SMD and those who support them (Fulfilling Lives, 2020).
- Treatment may be withdrawn from people who fail to attend appointments (Fulfilling Lives, 2020).
- People from ethnic minority backgrounds with experiences of SMD report that support services lack of role models of people who have had similar experiences to them (Robinson et al., 2017).
- Sex workers report discrimination from mental health services, including being excluded from services whilst continuing sex work, and a need for counsellors with an understanding of sex work (Mellor & Lovell, 2012).
- Changes to healthcare delivery during the earlier stages of the COVID-19 pandemic had mixed impacts (Groundswell, 2022a):
- Positive changes included some GPs switching from prescribing methadone daily, to doing so weekly or fortnightly. This helped increase patients’ trust with their GPs and allowed some people to access care who had previously struggled to engage with services.
- However, there were negative impacts on healthcare access for people who lacked access to digital devices or had low levels of digital literacy.
Individual barriers to accessing mental health support
- Being denied access to support can compound people’s past experiences of ‘failure, hopelessness and disappointment’, and make it less likely that they seek out mental health support in the future (Agenda, 2019).
- People from ethnic minority backgrounds with experiences of SMD report lacking trust in mental health services, including fears of being subject to negative stereotypes or of being sectioned (Robinson et al., 2017).
An example of the complex barriers and pathways to support people face is illustrated below:
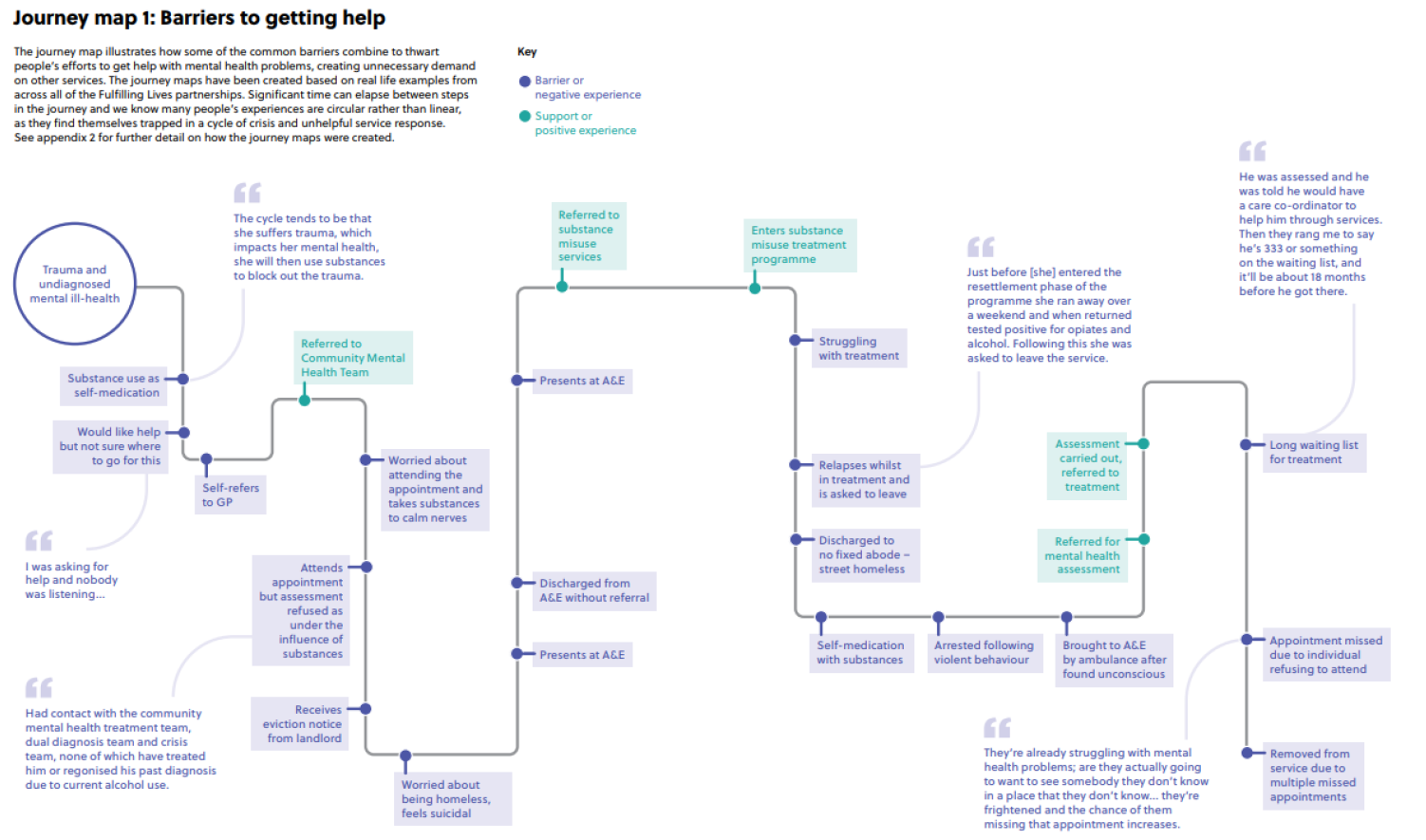
Figure 62: Journey map illustrating the barriers to accessing mental health support faced by someone experiencing SMD. Image source: Fulfilling Lives
Experience
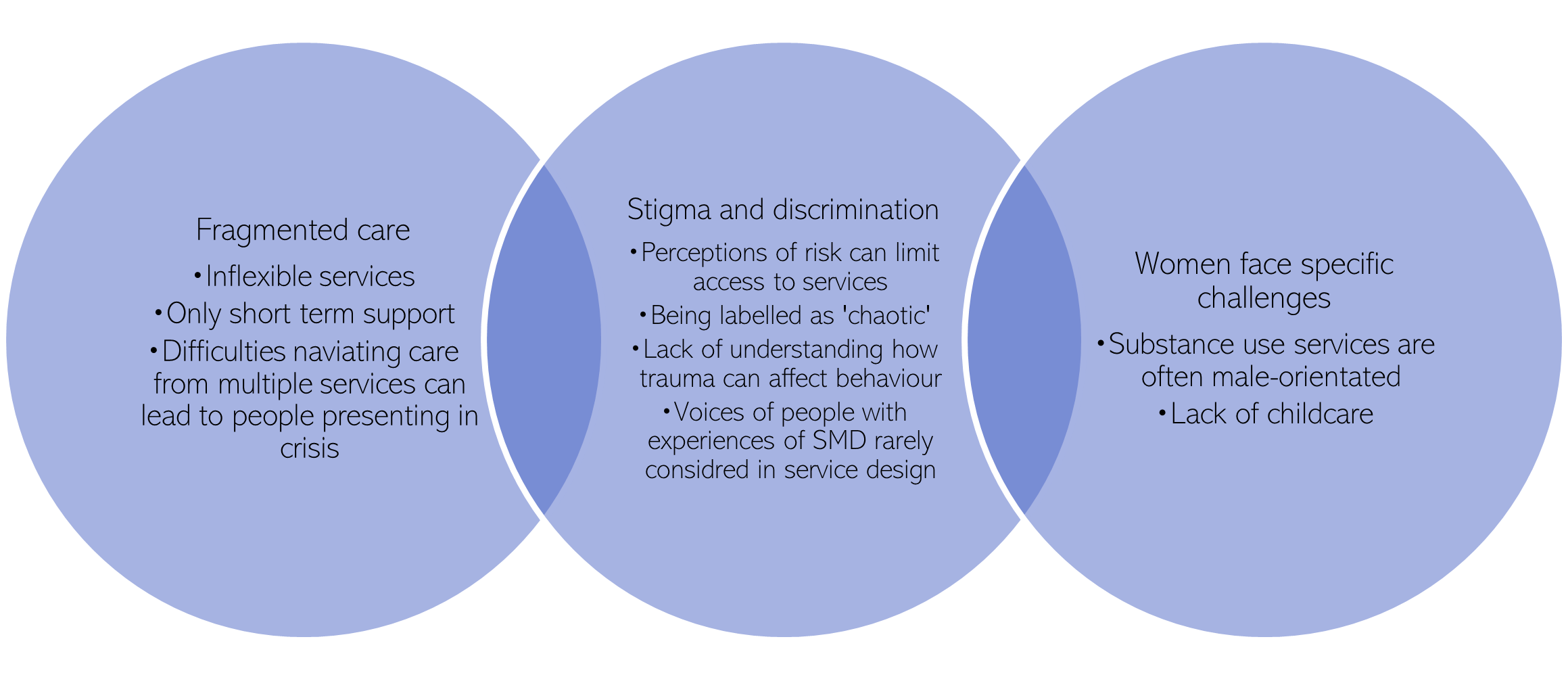
Figure 63: A summary of the experience of people with SMD when accessing mental health services
- People experiencing SMD often face high levels of stigma (Bramley et al., 2015). For example, a lack of understanding of SMD by healthcare professionals, including how trauma can affect behaviour, lead to people with SMD being labelled as ‘problematic, complex, chaotic, damaged or harmed’ [(Agenda, 2019),(Fulfilling Lives, 2020)]. A lack of understanding of the mental health needs of people facing SMD also occurs more widely, such as within the criminal justice system (Everitt & Kaur, 2019).
- People with complex needs often experience poor quality and fragmented care, as a result of navigating care from multiple services (Coleman, 2003).
- A lack of cross sector coordination means that people often end up falling through gaps between services, and ultimately ending up presenting in crisis (Coleman, 2003; Moreton et al., 2021).
- A lack of data sharing between services means that people experiencing SMD have to keep retelling their stories, which contributes to their ‘alienation’ from support systems (Everitt & Kaur, 2019).
- Most prisons take a ‘parallel approach’ to co-occurring conditions, in which patients are supported by multiple services simultaneously (Wright et al., 2016). This has been perceived as fragmented care and can pose challenges such as miscommunication between services (Wright et al., 2016).
- Support services accessed by people with SMD may offer support for a shorter period of time than is needed (Making Every Adult Matter Coalition et al., 2013).
- Women with SMD report that:
- That there is a lack of childcare services for young mothers receiving treatment for substance use (Bhonagiri & Senoran-Martin, 2021).
- There is a lack of assertive outreach services, which means people are more likely to disengage with services (Bhonagiri & Senoran-Martin, 2021).
- That healthcare professionals such as GPs often lack knowledge about services are available to support people with substance use (Bhonagiri & Senoran-Martin, 2021).
- Substance use services are often male-orientated, which can feel threatening for those who have experienced domestic abuse (Bhonagiri & Senoran-Martin, 2021).
- They may feel blamed for the situations they face (Agenda, 2019).
- The ways in which services respond to women experiencing SMD is ‘often based on gendered expectations of how men and women ‘should’ behave’ (Sosenko et al., 2020).
- The voices of people experiencing, or with experience of, SMD may not be considered in the design of services (Making Every Adult Matter Coalition et al., 2013).
Outcomes
‘The current system is not working for people facing multiple disadvantage. Many of their interactions with public services are negative and/or avoidable. Few receive the treatment they need.’ (Moreton et al., 2021)
- People facing SMD experience ‘profound health inequalities’ (Tweed et al., 2021) and have significantly higher rates of all-cause mortality than people who have experienced one type of deprivation (Tweed et al., 2021, 2022).
- The quality of life of people experiencing SMD is very poor, particularly in terms of mental health and social isolation (Bramley et al., 2015).
- People facing SMD are often not well supported by mainstream services (Moreton et al., 2021) and as result end up being ‘stuck in a revolving door’ around different support systems (Everitt & Kaur, 2019).
- ‘Blue light’ services such as crisis teams may be able to deal with immediate problems but are unlikely to recognise, or support people with, the underlying issues they experience (Everitt & Kaur, 2019).
- As a result, people experiencing SMD often have high levels of service use, with one estimate stating that this accounts to over £28,000 of public service use per person each year (Moreton et al., 2021)
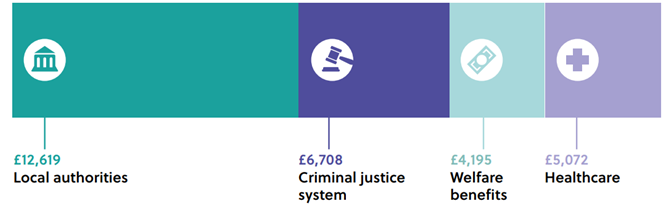
Figure 64: Average annual cost to public services of beneficiaries of the Fulfilling Lives programme, which supports people with SMD. Source: Fulfilling Lives
Additional resources
- The local data pack gives an overview of key data and trends
- Making Every Adult Matter‘s report Multiple disadvantage and co-occurring substance use and mental health conditions
- Hard Edges: Mapping severe and multiple disadvantage and Hard Edges: the lives behind the numbers, which details the life stories of people who have experienced severe multiple disadvantage
- A needs assessment produced by Nottingham City Council focusing specifically on SMD
- Changing Futures Cambridgeshire and Peterborough, a locally-funded programme supporting people with SMD. Five case studies are linked here: Mike , Gordon , Colin , Martin, Molly
- Improving access to mental health support for people experiencing multiple disadvantage
- Gender Matters: Gendered patterns of severe and multiple disadvantage in England
- Breaking Down the Barriers: Findings of the National Commission on Domestic and Sexual Violence and Multiple Disadvantage
- A Review of the Literature on Sex Workers and Social Exclusion
- Housing, Mental Health and Substance Misuse Toolkit
- Inclusion Health Self Assessment Tool for Primary Care Networks
- Inclusion Health: applying All Our Health
- NHS National Framework on Inclusion Health
- Homeless and Inclusion Health standards for commissioners and service providers
- Inclusion health data and intelligence resource for England – GOV.UK
Areas for future work
- Develop local estimates of severe multiple disadvantage at district level
References
Full list of references is included at the end of this chapter.