Inequalities
Research has consistently shown that there is a strong relationship between social disadvantage and poor mental health (Lancet, 2021). This was detailed in chapter two of the mental health needs assessment. There are also links between unhealthy relationships and loneliness, and poor mental health: hence relationships are a key priority in the local Health and Wellbeing Integrated Care Strategy.
- It is well recognised nationally that some groups are more likely to experience serious mental illness, and that many of these groups also face barriers preventing timely access to care (Davidson, 2021). This can be seen in terms of the unequal use of crisis care in the local pathway.
- Getting It Right First Time (GIRFT) has documented that across the country while the ethnic breakdown of those accessing core services may be similar to the overall population mix, the proportion of people from Black, Asian and other minority ethnic backgrounds is disproportionately high among in higher-intensity forms of community and inpatient services (Davidson, 2021).
- GIRFT states that both the inpatient admission and community caseload data related to ethnicity provide a stark illustration of the fact that if services do not get things right at the beginning, people will disproportionately end up in longer-term and/or more restrictive settings owing to avoidable extra acuity and the accumulation of preventable secondary and tertiary problems (Davidson, 2021).
One way of assessing inequalities in terms of access to mental health services is to compare who is accessing mental health support compared to our local population. Understanding barriers is important to addressing inequalities and is linked to the local Health and Wellbeing Strategy priority around ‘motivation’ and removing barriers to accessing services. These graphs give a broad overview of inequalities in access to mental health services. However, it is also important to note that some variations may be due to differences in mental health need. Different groups are more likely to experience mental illness (NHS Digital, 2014), due to a complex range of biological, social and economic factors.
Gender
A greater proportion of women than men access Talking Therapies, CPFT’s Primary Care Mental Health Service (PCMHS) and the First Response Service (FRS).
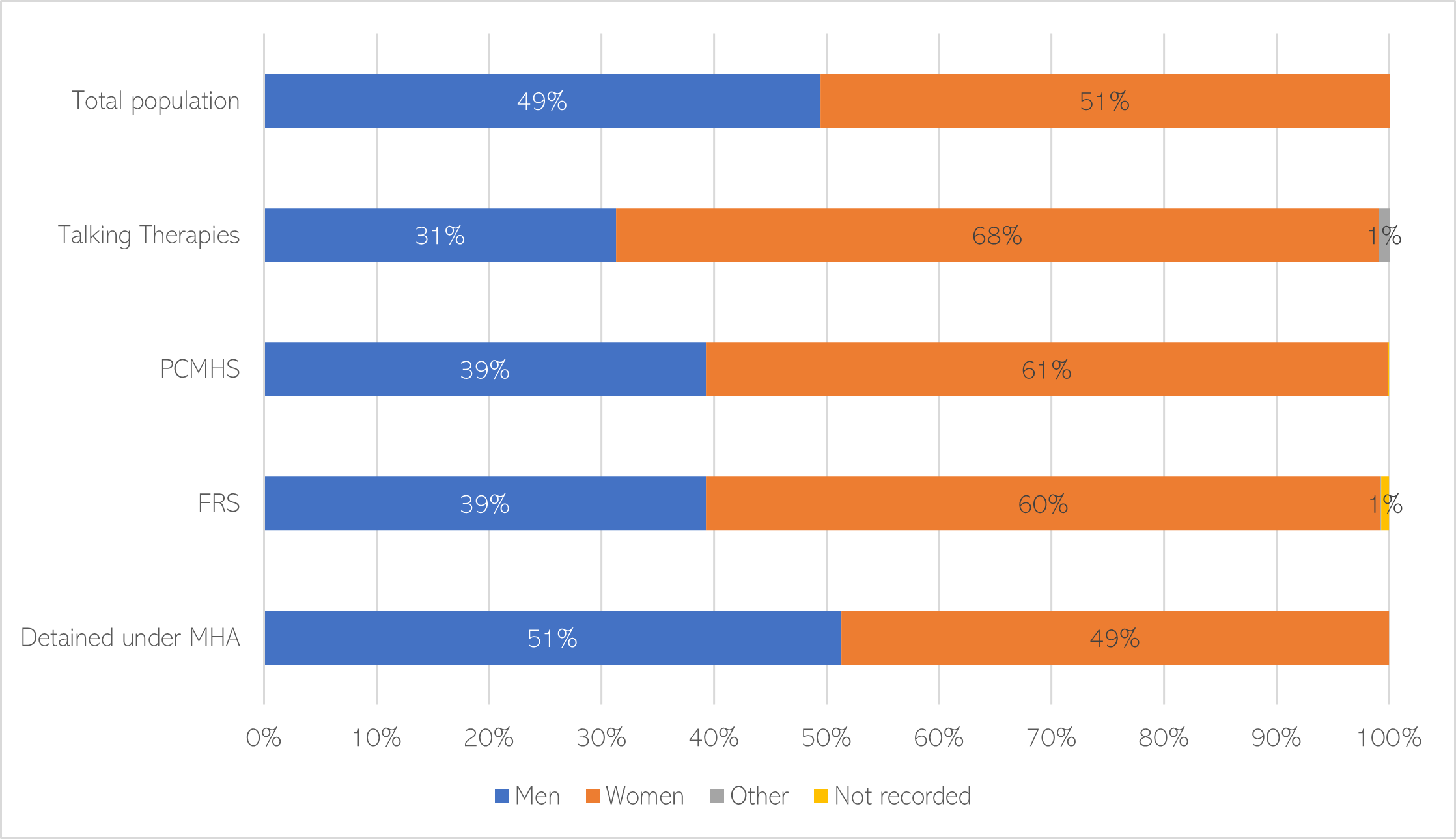
Figure 20: Access to mental health services in Cambridgeshire and Peterborough by gender. Data sources listed above.
Ethnicity
From this analysis, it seems that people from Black, and Asian ethnic groups are more likely to be detained under the Mental Health Act than their White counterparts. This would reflect national data trends (Weich et al., 2020); however, it is difficult to draw conclusions from local data due to missing or unrecorded ethnicity data. The use of broad categories for ethnicity will have masked differences within groups. For example, national analyses highlight people from ‘Bangladeshi’ ethnic groups are the least likely to receive treatment from NHS Talking Therapies (National Collaborating Centre for Mental Health, 2023).
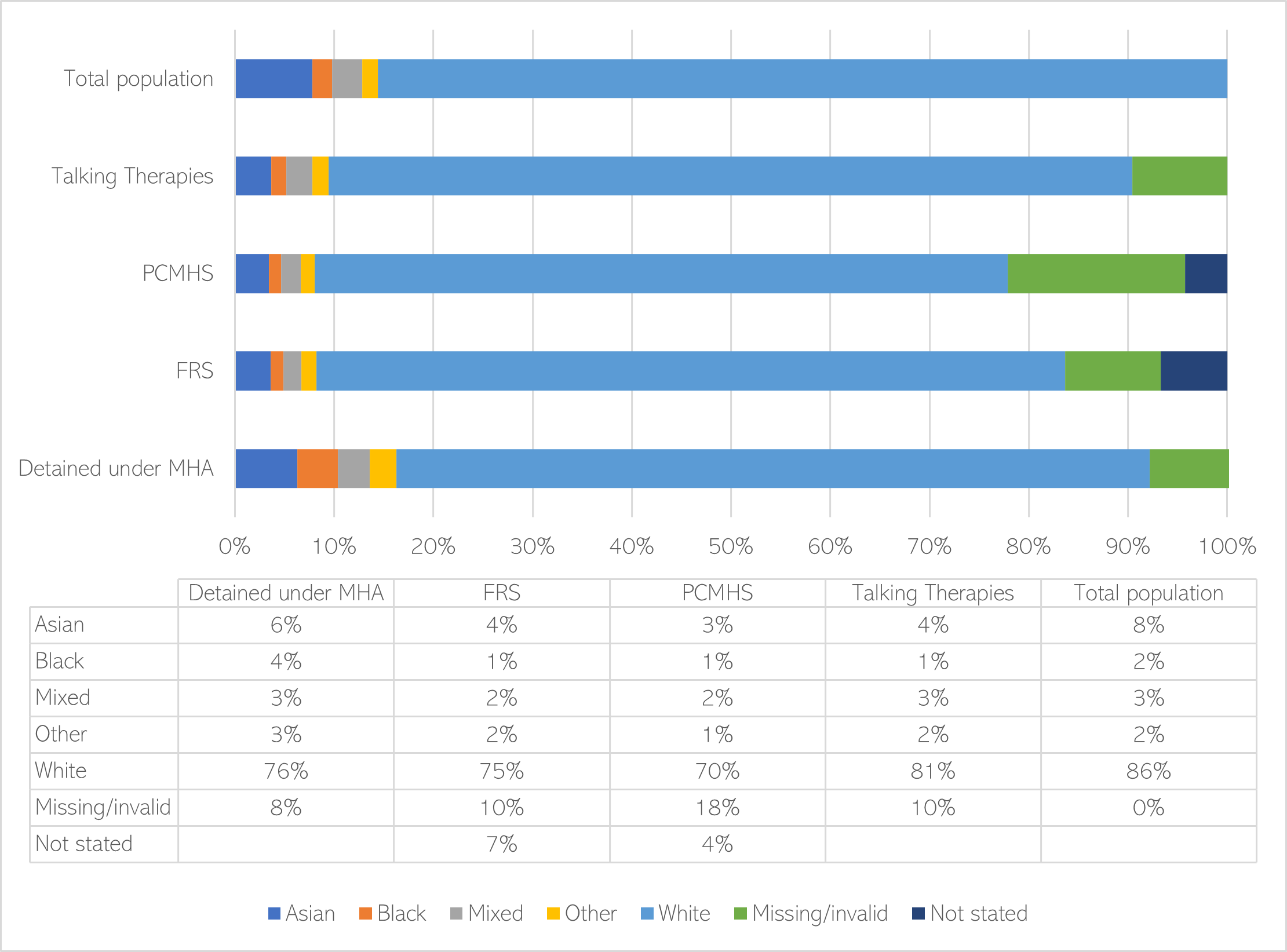
Figure 21: Caseload of mental health services in Cambridgeshire and Peterborough ICS, by ethnicity. Data sources listed above
Deprivation
People living in the most deprived areas of Cambridgeshire and Peterborough are more likely to present to mental health services, particularly the Primary Care Mental Health Service (PCMHS) and the First Response Service (FRS).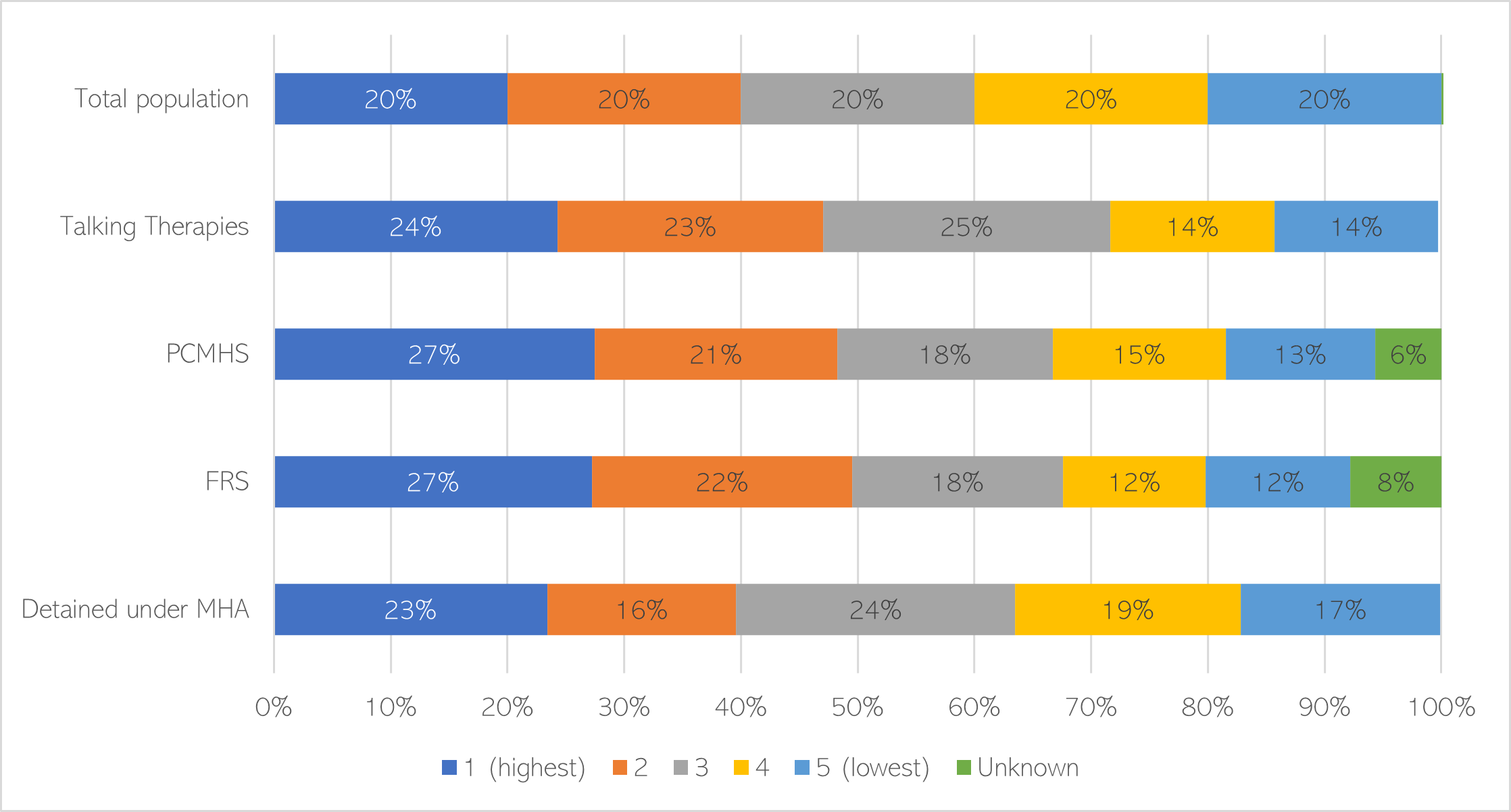
Figure 22: Caseload of mental health services in Cambridgeshire and Peterborough ICS, by local deprivation quintile. Data sources listed above
Data sources and caveats
Data covering Cambridgeshire and Peterborough was analysed from a range of sources:
- Total population
- https://cambridgeshireinsight.org.uk/jsna-2023/demography/age-structure-and-population-change/
- Data collected as part of the 2021 Census
- Talking Therapies
- https://digital.nhs.uk/data-and-information/publications/statistical/psychological-therapies-annual-reports-on-the-use-of-iapt-services/annual-report-2021-22
- Referrals accessing services in 2021/22
- Primary care mental health service (PCMHS)
- Analysis carried out from CPFT data, for the Mental Health Needs Assessment
- Analysis of unique referrals accessing PCMHS, January 2019 – July 2023
- First Response Service (FRS)
- Analysis carried out from CPFT data, for the Mental Health Needs Assessment
- Analysis of unique referrals accessing FRS, August 2021 – March 2023
- Detained under the Mental Health Act
- MHA Dashboard – Mental Health, Learning Disability and Autism Resource Hub – FutureNHS Collaboration Platform
- Detentions under all sections of the Mental Health Act, July 2022 – June 2023
Caveats to this analysis include:
- Data was collected over different time periods, which may have distorted the findings.
- There is a lack of intersectional analysis, which considers the impact of multiple demographic factors on access to services, such as the interaction of age, gender and ethnicity. Some factors, such a deprivation, may underlie differences between groups.
- Some data, particularly for ethnicity, is missing from the datasets analysed. This prevents a full understanding of service use.
Additional resources
- The local data packs give an overview of prevalence and service use
- Chapter two of this mental health needs assessment covers inequalities in mental health services in more detail, covering access, experience and outcomes
References
Full list of references is included at the end of this chapter.