Life stages
Children and young people navigate a range of changes during their lives, including through the education system. These transition points can provide opportunities for children and young people’s growth and learning but can also have a negative impact on their lives, particularly if they have multiple stressors in their lives (Bagnall et al., 2022).
This section will consider the mental health and wider needs of children and young people broken down into four key age groups: preschool (age 2 to 4); primary school (age 5 to 10); secondary school (age 11 to 16); and entering adulthood (age 17 to 25). It will also consider what works to promote good mental wellbeing in children and young people. More detailed data is included in the Children and Young People Mental Health Dashboard.
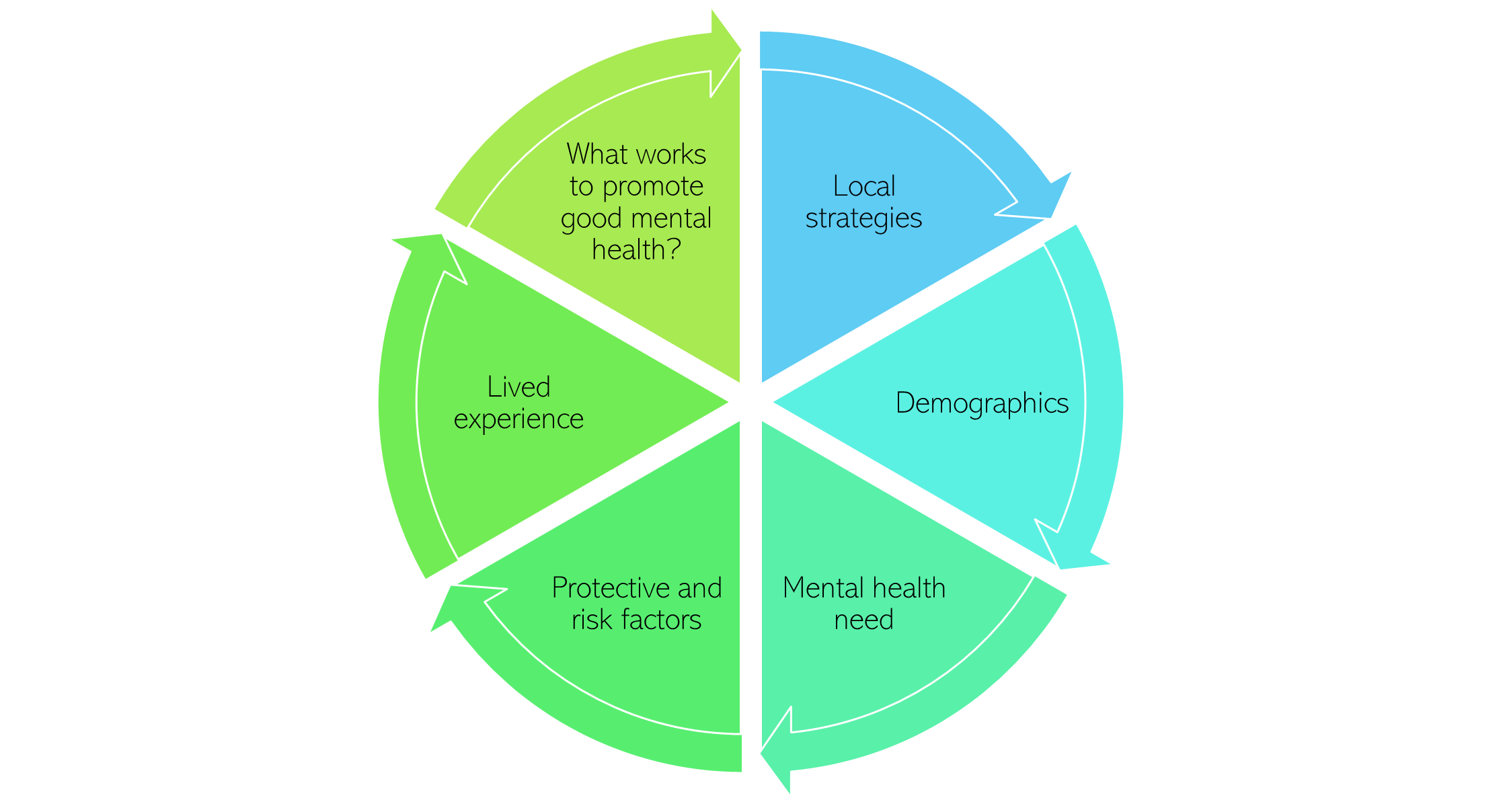
Figure 8: Structure of this section of the needs assessment
Protective and risk factors
These sections include prevalence of risk and protective factors in Cambridgeshire and Peterborough. The negative impact of risk factors on a child or young person can be counteracted by protective factors, such as the presence of a supportive adult (Public Health England, 2019b).
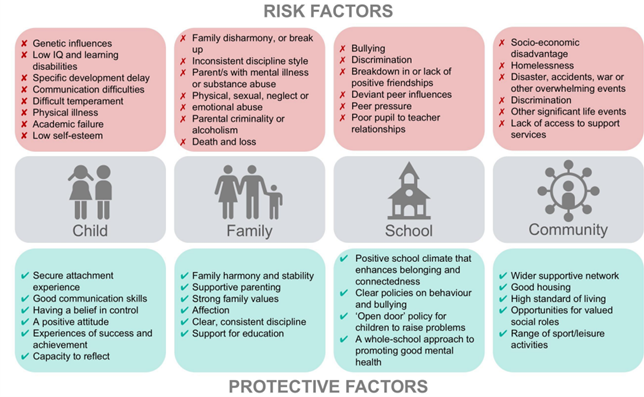
Figure 9: Risk and protective factors for children and young people’s mental health. Image source: Public Health England
Some protective and risk factors, such as family, poverty and adverse childhood experiences, run across all age groups.
Adverse childhood experiences
Adverse childhood experiences (ACEs) are a ‘a set of 10 adverse experiences in childhood which are associated with an increased risk of poor health and other problems in later life’ (Asmussen et al., 2020). They range from common experiences (such as parental separation) to horrific experiences (such as abuse) and typically identified as 10 experiences, including those (Asmussen et al., 2020; Felitti et al., 2019):
- Directly related to young people: physical abuse, psychological abuse, sexual abuse, physical neglect, psychological neglect.
- Related to their household: parental separation/divorce, having a close family member with a mental health condition, having a close family member spend time in prison, witnessing domestic abuse, and having a close family member with harmful drug or alcohol use.
However, recent UK research has also included living in households where a parent has died, spending time in care, and experiencing homelessness as ACEs (Lester et al., 2019).
Figure 10: 10 key adverse childhood experiences. Image source: Liverpool CAMHS
Most young people are resilient to experiences of adversity or will recover from the initial symptoms of poor mental health over time (Yule et al., 2000). However, exposure to prologued or severe ACEs can trigger ‘toxic stress’, which is an extreme level of stress that can have damaging impacts on health across the lifespan (Nelson et al., 2020; UNICEF, 2021a). The cumulative impact of adverse experiences is an important risk factor for poor mental health (Kessler et al., 2010), with individuals who have multiple ACEs being many more times likely to develop mental health conditions and substance use. Almost a third of all mental health conditions in adulthood are directly connected to an ACE (Kessler et al., 2010). Compared to experiencing no ACEs, an adult who experienced four or more ACEs is (Public Health England, 2019b):
- 4 times more likely to be a high-risk drinker
- 11 times more likely to have smoked cannabis
- 16 times more likely to have used heroin or crack cocaine
It is important to note that ACEs do not cover all childhood risk factors for poor mental health; or exist in isolation (Asmussen et al., 2020). Exposure to one ACE is a risk factor for experiencing subsequent ACEs, which means that the burden of ACEs (and associated outcomes) disproportionately impacts some individuals (Felitti et al., 2019). On top of this, many ACEs are linked to social inequalities such as poverty and deprivation, with children from lower socioeconomic backgrounds being at higher risk of experiencing ACEs (Bellis et al., 2014; Walsh et al., 2019). Recent research has also suggested that parental conflict, and how this is expressed and managed, may be more important to child outcomes than divorce (G. T. Harold & Sellers, 2018). This suggests that exposure to ACEs may be less informative without also understanding the wider context of this experience.
Early interventions to help the mental health of young people who have experienced adverse childhood experience – Interventions to address ACEs
What is the local picture?
- By age 18, 40 to 60% of the population will have experienced a single ACE and 4 to 20% will have experienced four or more ACEs (Asmussen et al., 2020). One estimate is that that 15,000 children in Cambridgeshire and Peterborough have experienced four or more ACEs (Cambridgeshire and Peterborough Integrated Care System, 2022f).
- The prevalence of ACEs is estimated to be highest in areas with higher rates of child poverty. One study which ranked English local authorities by the estimated prevalence of ACEs suggests that there is a much higher prevalence of ACEs in Peterborough, and much lower in East Cambridgeshire, South Cambridgeshire, and Huntingdonshire (Lewer et al., 2020).
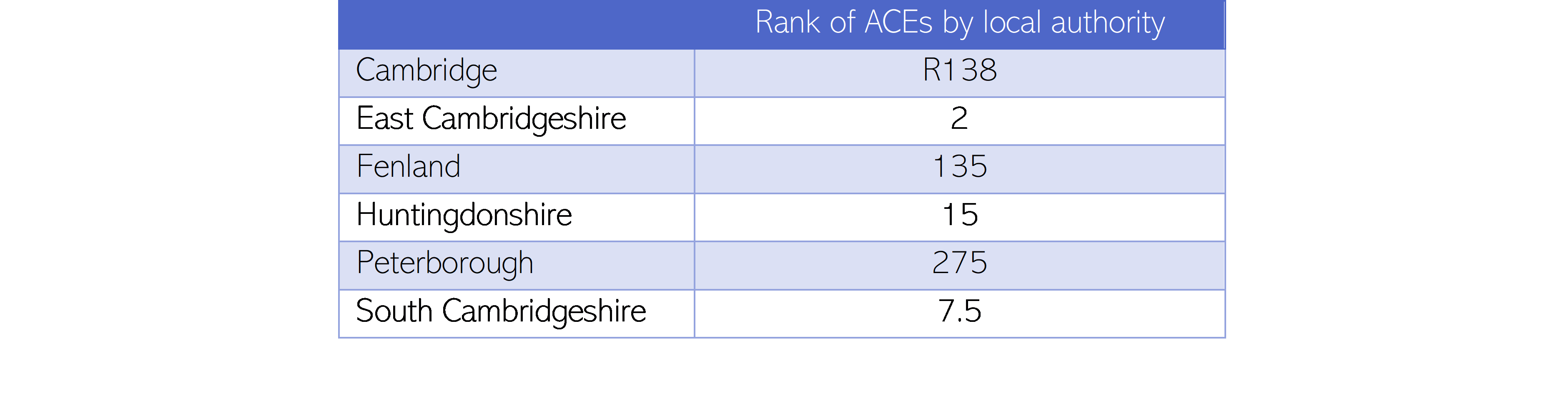 Table 5: ACE ranking (ranking between 1 and 324, where 1 indicates the local authority with the lowest estimated prevalence of ACEs in England, and 324 the local authority with the highest prevalence) across Cambridgeshire and Peterborough, 2020. Data source: (Lewer et al., 2020)
Table 5: ACE ranking (ranking between 1 and 324, where 1 indicates the local authority with the lowest estimated prevalence of ACEs in England, and 324 the local authority with the highest prevalence) across Cambridgeshire and Peterborough, 2020. Data source: (Lewer et al., 2020)
There is some data on the number of children and young people with specific ACEs:
- It is estimated that 29,000 children and young people in Cambridgeshire and Peterborough live or have lived in couple-parent families whose parents had a ‘distressed relationship’ (Cambridgeshire and Peterborough Integrated Care System, 2022f). A couple-parent family is classified as experiencing relationship distress if either parent reports that ‘most or all the time they consider divorce, regret living together, quarrel, or get on each other’s nerves’ (Department for Work and Pensions, 2022).
- In 2020/21, there were 442 children (under 18s) on child protection plans in Cambridgeshire, and 285 in Peterborough. This means that they were at ‘continuing risk of significant harm’ due to physical, emotional or sexual abuse, or neglect. The rate of children on child protection plans is similar to the national average in both Cambridgeshire and Peterborough.
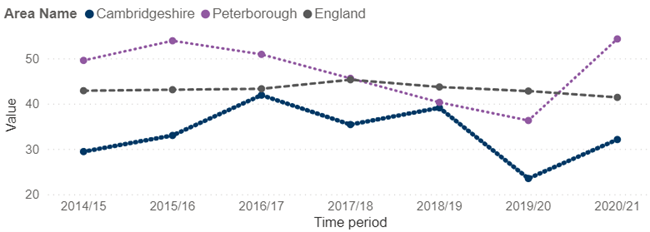
Figure 11: Rate of children (aged under 18) on child protection plans, per 10,000, from 2012/13 to 2020/21. Data source: Fingertips. Note: Children are put on child protection plans if they are at continuing risk of ‘significant harm’, as a result of physical, emotional or sexual abuse, or neglect.
- The rate of children in households with a combination of parental alcohol and drug problems, parental severe mental illness (SMI) and domestic abuse is higher than the national rate in Cambridgeshire and Peterborough.
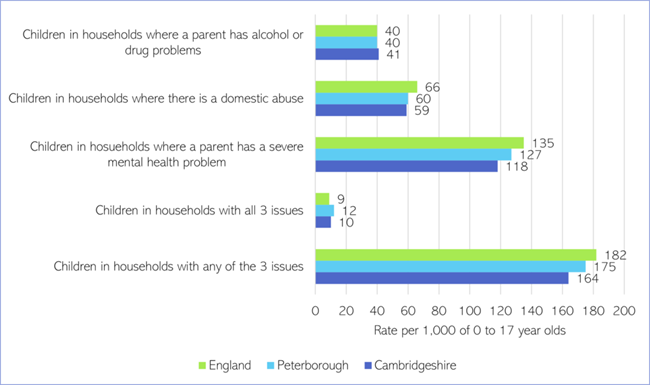
Figure 12: Prevalence of parental substance use, mental ill health and domestic abuse. Source: Parents with problem alcohol and drug use: Data for England, Cambridgeshire and Peterborough, 2019 to 2020, NDTMS.
Additional resources
- Adverse childhood experiences: What we know, what we don’t know, and what should happen next
- Addressing childhood adversity and trauma
- Adversity in childhood is linked to mental and physical health throughout life
References
Full list of references is included at the end of this chapter.