Funding and Economics
For the past five years, per head spend on across all mental health services (adjusted for mental health need) has been below the national average in Cambridgeshire and Peterborough. These figures include spending on all-age mental health services, as well as learning disability and dementia services.
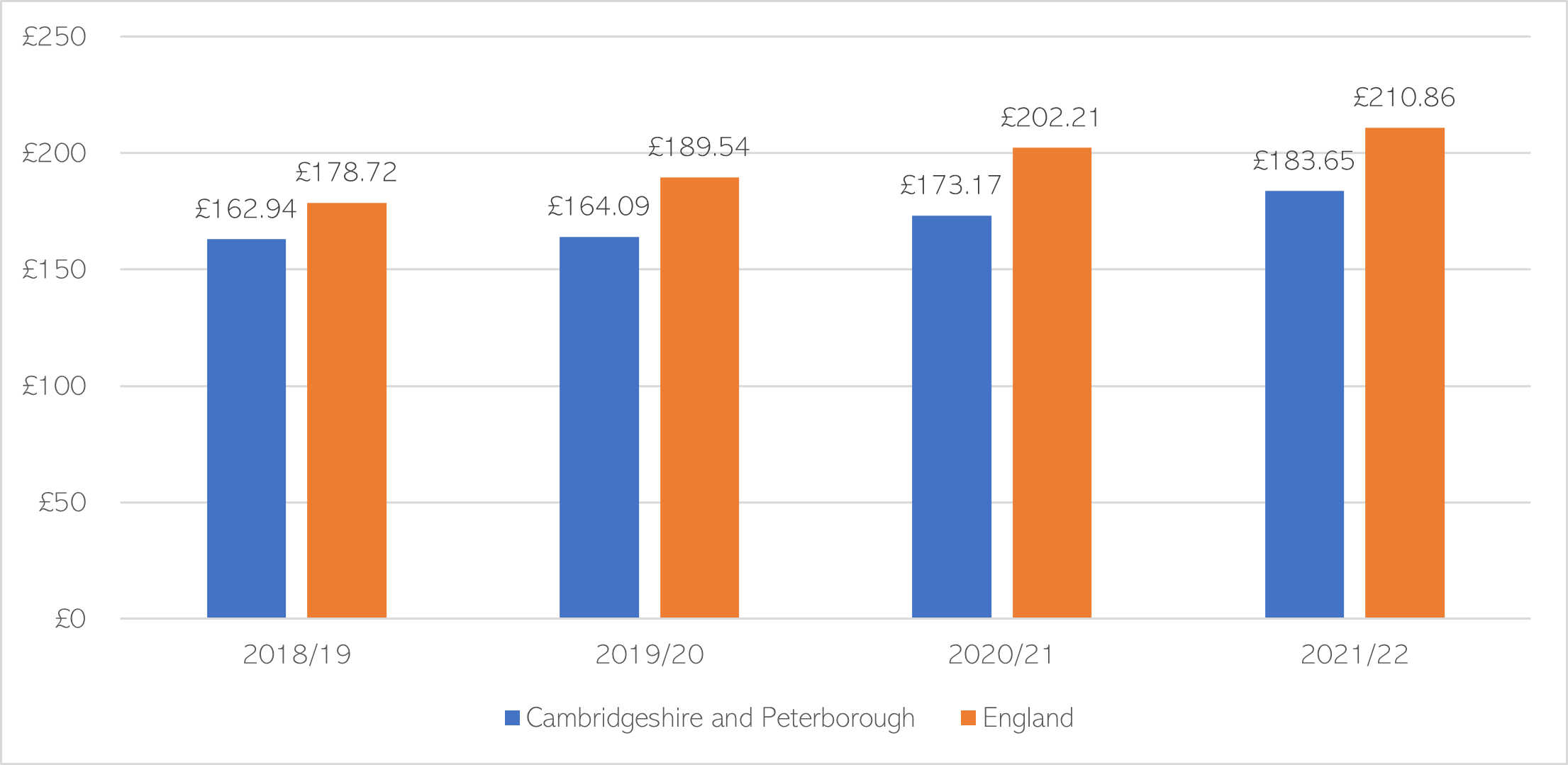
Figure 28: Per head spending on mental health services in Cambridgeshire and Peterborough, adjusted for mental health need. Data source: Royal College of Psychiatrists. Note: this data is standardised to take account of mental health need using NHS England needs-based population data for 2018/19 – 2021/22.
Getting It Right First Time (GIRFT) recommends that trusts work with system partners to ensure that the Mental Health Investment Standard is met, and that they have nominated finance/transformation leads at senior level with a thorough understanding of the Standard and can specifically identify the growth in investment expected in each service area (Davidson, 2021)
Health economics
- Although health economics is used to inform decision making across healthcare systems, this has historically been underused within mental health (Lathe et al., 2023).
- Some argue that economic estimates of the impact of mental health conditions often underestimates their true costs. Mental ill health may have a range of impacts on society, including on interpersonal relationships, education, employment and benefits, social services, other areas of the healthcare system and the criminal justice system (Lathe et al., 2023; Watson, n.d.).
- In a 2023 review of mental health services in England, the National Audit Office highlighted that ‘understanding of costs of services is still poor for many areas, including in primary and community services’ (House of Commons Committee of Public Accounts, 2023).
The World Health Organisation has proposed that frameworks analysing the impacts of investing in mental health services should consider health impacts (e.g. on both physical and mental health), social impacts (e.g. on social functioning and carers) and financial impacts (e.g. on employment and physical health care costs) (World Health Organisation, 2021). However, the scope of analyses and the availability of data varies across these domains.
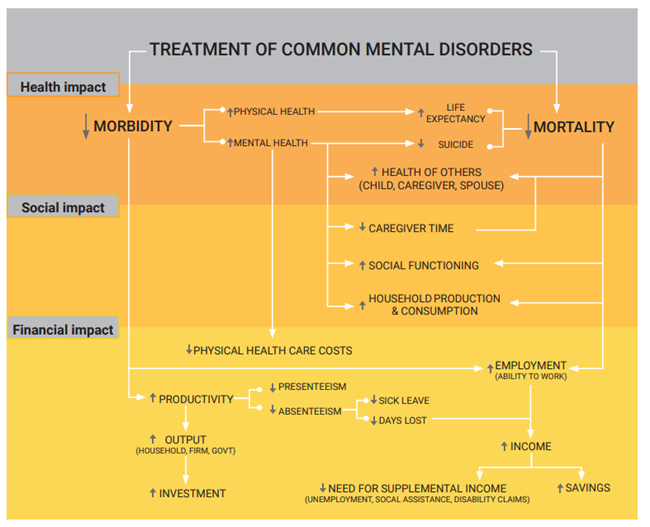
Figure 29: Analytical framework for identifying potential impacts of mental health investment. Image source: World Health Organisation
Additional resources
- The economic and social costs of mental ill health
- Oxford Mental Health Economics and Policy
- Mental Health Investment Standard (MHIS) categories
- The economic case for investing in the prevention of mental health conditions in the UK
- Mental health promotion and mental illness prevention: The economic case
- Better Mental Health For All
- Mental health investment case: a guidance note
- Public mental health: Evidence, practice and commissioning (see pages 109 – 114)
- The Economic and Social Costs of Mental Ill Health
References
Full list of references is included at the end of this chapter.