Inequalities in mental health
There are well-established risk factors for poor mental health in young people. These factors were detailed in the Children and Young People’s Mental Health Strategy (Cambridgeshire and Peterborough Integrated Care System, 2022f) and the Mental Health and Wellbeing Pre-birth to Age 25 years Needs Assessment November 2019 (Hedges et al., 2019).
- NHS England has developed CORE20PLUS5 model to understand health inequalities. ‘Improving access rates to children and young people’s mental health services for 0–17-year-olds, for certain ethnic groups, age, gender and deprivation’ is a key priority of this model (NHS England, 2023a)
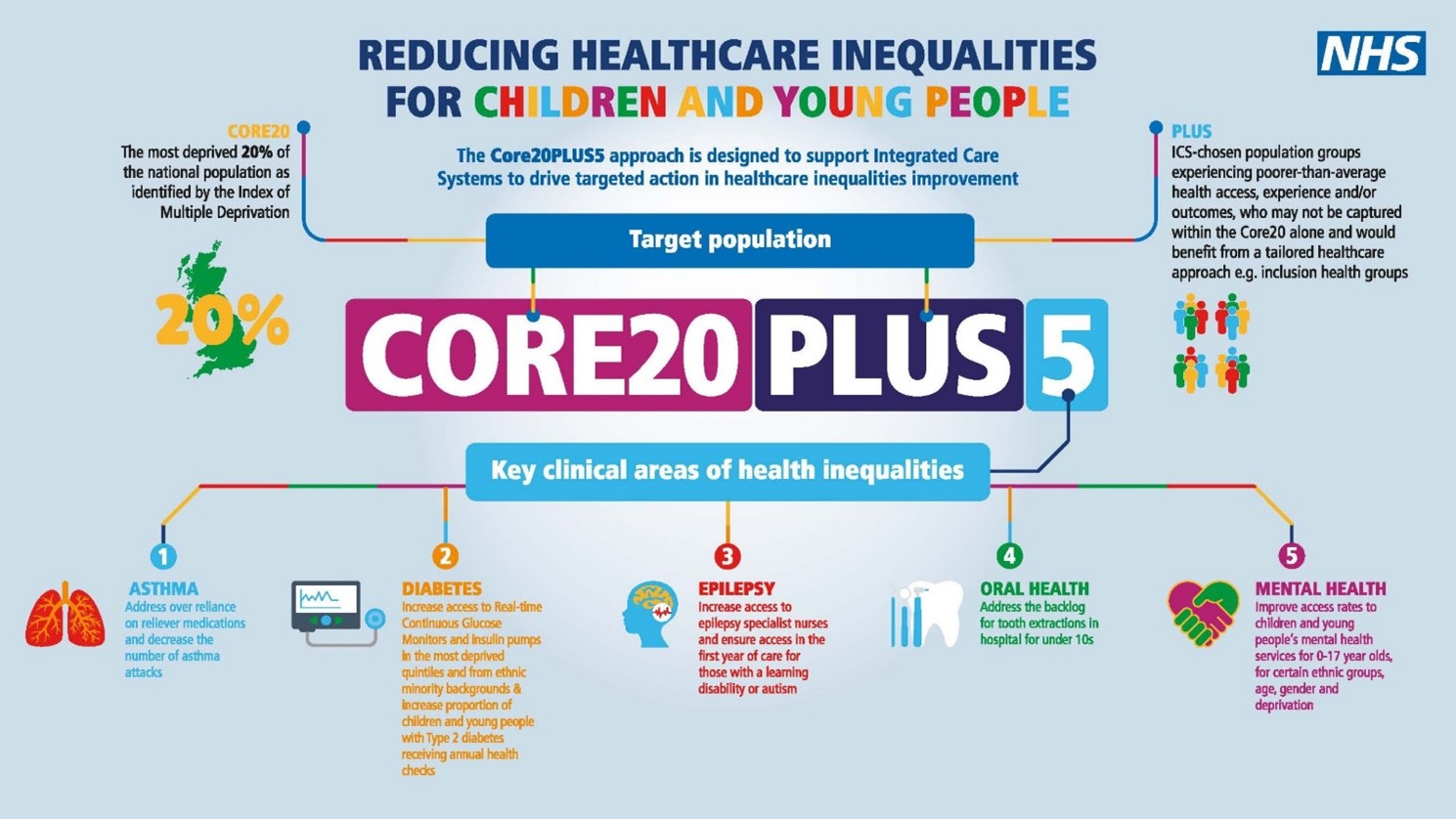
Figure 28: CORE20PLUS5 model for understanding healthcare inequalities for children and young people. Image source: NHS England
Chapter One of this needs assessment includes more information on relevant wider determinants of health in Cambridgeshire and Peterborough. Chapter Two covers population groups that are more likely to experience inequalities in mental health, in terms of: increased risk of experiencing mental health conditions, risk factors, and inequalities in the access, experience and outcomes from mental health services. This chapter (Chapter Three) covers adverse childhood experiences.
Socioeconomic deprivation
- Deprivation: 1 in 5 children in Peterborough and Fenland live in income deprived households, which is a significantly higher level than the national average (Office for Health Improvement and Disparities, 2022).
- Poverty and financial insecurity: there are over 25,000 children (under 16s) in Cambridgeshire and Peterborough living in low income families (Office for Health Improvement and Disparities, 2022)
Equality and diversity
- Gender: national data shows that 1% of 16- to 24-year-olds are transgender (Office for National Statistics, 2022a). There is a lack of data on younger age groups.
- Sexuality: national data states that 7% of 16- to 24-year-olds are LGB+ (Office for National Statistics, 2022c). There is a lack of data on younger age groups.
- Refugees and asylum seekers: there is a lack of local data on the number of children who are refugees or seeking asylum (Cambridgeshire and Peterborough Integrated Care System, 2022f).
- Disability: there are 19,000 school pupils in Cambridgeshire and Peterborough with a statutory special education need (SEN) plan or receiving SEN support (Cambridgeshire and Peterborough Integrated Care System, 2022f).
- Learning disability: The mental health needs of children and young people with learning disabilities will be covered in the Cambridgeshire and Peterborough Learning Disabilities Needs Assessment (published in 2024).
- Neurodiversity: it is estimated that there are over 2,700 autistic people aged between 5 and 24 in Cambridgeshire and Peterborough (Cambridgeshire County Council & Peterborough City Council, 2021). There will be a specific chapter of the mental health needs assessment focusing on neurodiversity (published in 2024).
- Care experienced people: in 2022, there were 597 children in care in Cambridgeshire and 354 children in care in Peterborough (LG Inform, 2022).
- Young carers: it is estimated that there are 5,000 young carers aged between 11 and 17 in Cambridgeshire and Peterborough (Cambridgeshire and Peterborough Integrated Care System, 2022f).
- Ethnicity: 30% of school pupils in Cambridgeshire and 56% in Peterborough classified themselves as belonging to an ethnic group other than White British in the 2022/23 school year (Department for Education, 2023b).
Mental Health Needs of Ethnically Diverse Children and Young People Including Young Refugees and Asylum Seekers.
Children and young people from ethnically diverse backgrounds, including refugees and asylum seekers, face unique challenges that affect their mental health. These groups are often underrepresented in service design and delivery, and their experiences are not always reflected in current support models.
Key Findings:
- Underrepresentation: Ethnically diverse CYP are less likely to have their voices heard in mental health services. Their lived experiences are often missing from service planning.
- Professional insight: We gathered feedback from professionals working closely with these groups to better understand their needs and the barriers they face, including youth workers, community leaders, and the VCSE sector to better understand their needs and the barriers they face.
- Cultural sensitivity: Services must reflect the cultural contexts of these young people to be effective.
Our approach to understanding the issue is based on lived experience data. We drew this insight from a variety of sources, such as case studies, community feedback, and interviews with practitioners.
Mental Health and SEND Support in the Muslim Community
Families in the Muslim community, particularly those with children who have SEND or mental health needs, face specific challenges. Cultural attitudes towards mental health and neurodiversity can delay early identification and access to support.
This insight is based on lived experience data gathered from a former cohesion manager at Peterborough City Council and an organisation called Julaybib, who have direct knowledge of the barriers faced by families in the local area.
Key Findings:
- Stigma and fear: Parents, especially of girls, may fear social consequences if they seek help. This can lead to delayed intervention.
- Gender differences: Girls may feel restricted by cultural expectations, while boys may not recognise or acknowledge their difficulties.
- Peer support: Trusted, community-led peer support is often the most effective way to build understanding and encourage help-seeking.
Mental Health Needs of Young Refugees and Asylum Seekers
Young refugees and asylum seekers often experience trauma and face significant barriers to accessing mental health support.
This insight is based on lived experience data gathered from BACA, an organisation who work directly with young refugees and asylum seekers.
Key Findings:
- Language and cultural barriers: Talking therapies may not be suitable due to language limitations and cultural norms around mental health.
- Creative therapies: Approaches like dance and art therapy have proven effective in helping young people express their experiences.
- Service limitations: Traditional services like CAMHS can be inflexible and time-limited, which does not meet the complex needs of this group.
- Trust and relationships: Building trust takes time. In-house therapy models, like those used by Baca, allow for more consistent and personalised support.
Insights from the Cambridge Youth Forum
Principles, Themes, and Challenges in CYP Mental Health Support
To better understand young people’s views on mental health support, we engaged with the Cambridge Youth Forum, coordinated by a CPFT-employed facilitator. Around 70% of forum members are from the Global Majority, offering valuable perspectives from a diverse range of lived experiences.
Key Principles for Mental Health Support:
Forum members identified the following as essential features of effective support:
- Welcoming environments: Services should feel friendly, warm, and non-clinical.
- Inclusivity: Support must meet the needs of all young people, without judgement.
- Accessibility: Services should be local, school-based, community-led, and available in multiple formats, including 24/7 crisis support.
- Holistic care: Mental health support should consider wider life issues like relationships and school stress.
- Continuity: Ongoing support is needed beyond crisis points.
- Knowledgeable staff: Professionals should be well-informed and able to guide young people to the right help.
- Trusted assessments: Young people should only need to tell their story once to avoid re-traumatisation.
Key Themes:
- Schools as a hub: Schools play a central role in both delivering support and promoting mental health awareness. Staff training and visible signposting are essential.
- Digital options: Young people value virtual support, text-based services, apps, and online resources.
- Safe spaces: Home is not always a suitable setting. Dedicated mental health spaces in schools and clinics are needed.
- Support networks: Involving family, peers, school staff, and professionals is vital. Effective information sharing helps build a strong support system.
Challenges Identified:
- Lack of awareness: Many young people don’t know what support is available.
- Information sharing and consent: These processes can be confusing and act as barriers.
- Age-appropriate services: There are gaps in tailored support for different age groups.
- Support for non-school attendees: Young people who are home-schooled or not in education need better access to services.
Key Recommendations
Source of Recommendations
The following recommendations were developed following interviews and engagement with professionals and organisations who work directly with ethnically diverse children and young people, including refugees and asylum seekers. Their insights were crucial in identifying the challenges and shaping practical, culturally sensitive solutions.
Organisations consulted include:
- Baca – supporting unaccompanied young refugees and asylum seekers
- Julaybib – a Peterborough-based charity supporting families in the Muslim community
- Cambridge Youth Forum – facilitated by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT), with strong representation from the Global Majority
- Culturally Sensitive and Trauma-Informed Care
- Train professionals in cultural competence and trauma-informed practice.
- Design services that respect cultural norms and family dynamics.
- Bridging Language and Communication Gaps
- Provide interpreters and multilingual therapists.
- Use creative therapies (e.g. art, dance) for non-verbal expression.
- Flexible and Accessible Services
- Make mental health services for children and young people more adaptable to young people’s circumstances.
- Expand community-based and school-based support options.
- Building Trust and Relationships
- Support long-term therapeutic relationships.
- Fund community-led and peer-to-peer support initiatives.
- Raising Awareness and Improving Information Sharing
- Create culturally appropriate resources to inform families and young people.
- Improve consent and data-sharing processes across services.
- Strengthening the Role of Schools
- Train school staff to identify and respond to mental health needs.
- Position schools as safe spaces for early intervention and support.
Gypsy, Roma and Traveller (GRT) Children and Young People (CYP)
GRT children and young people face unique mental health challenges linked to discrimination, exclusion, and cultural barriers. These factors contribute to mistrust of services and underrepresentation in support planning. Despite clear risks, there is a lack of lived experience data, making it difficult to design effective, culturally sensitive services.
The insights presented in this section are primarily drawn from interviews and conversations with professionals who work directly and regularly with Gypsy, Roma and Traveller (GRT) communities in Cambridgeshire and Peterborough. These include members of Cambridgeshire County Council’s Communities Team, a former Healthwatch Cambridgeshire and Peterborough project lead, and staff attending local GRT drop-in sessions. Their lived experience and frontline observations form the foundation of this analysis, highlighting limited professional engagement and the need for targeted support. These findings are supported by external research and national data where available.
Recording GRT Identity in Health Data
Many GRT individuals do not disclose their ethnicity due to mistrust, poor treatment, and lack of appropriate options on forms. Practical barriers like literacy and digital exclusion also play a role.
This under-reporting creates gaps in health data, making it harder to identify and respond to needs—particularly around mental health and suicide risk in young people. Services must build trust, improve data collection methods, and ensure respectful engagement to better support GRT communities.
See: Equitable data collection for Gypsy, Roma and Traveller communities in health services
Suicide Risk Among Young Men in GRT Communities
Young men from GRT communities face a significantly higher risk of suicide than the general population. Although UK suicide statistics do not record ethnicity, research from Ireland shows that Irish Travellers—particularly young men aged 15–25—account for 10% of national young adult male suicide statistics, despite making up less than 1% of the population.
See: Mental Health Needs Assessment suicide and self harm page.
See: Reaching for the rope, mental health in GRT communities.
Local Context: Cambridgeshire and Peterborough
- Young men aged 15–25 are already recognised as a high-risk group in local suicide audits [2].
- Peterborough, with high deprivation and a large GRT population, records higher suicide rates, especially among men [2].
- Interviews suggest GRT young men often face early pressure to provide for their families, contributing to mental health strain [1].
Severe multiple disadvantage
‘The young people we are focusing on are unlikely to self-diagnose mental health difficulties or self-refer themselves for treatment and help. Already under extreme pressure, often struggling with school and most at risk of being targeted by those wishing to exploit them, these young people need mental health support that seeks them out, delivers in a way that meets their needs in the community and is there for the long term.’ – Children and Young People’s Mental Health Coalition (Children and Young People’s Mental Health Coalition & Centre for Mental Health, 2022)
- Contact with the criminal justice system, including the wider needs of young offenders: there were 119 first time entrants to the youth justice system (aged 10 to 17) in 2021 (Office for Health Improvement and Disparities, 2022).
- Homelessness: 2381 young people (aged 16 to 24) in Cambridgeshire and Peterborough approached by their local authority because they were homeless, or at risk of being homeless, in 2021/21 (Centrepoint, 2023).
- Victims of crime: national data suggests that 12.0% of children under 12, and 18.4% of young people aged 11 to 17, have witnessed domestic abuse or threatening behaviour at home (Moroz, 2021).
- Substance use, including parental substance use: there were 185 hospital admissions due to substance use in young people (aged 15 to 24) from 2018/19 to 2020/21 (Office for Health Improvement and Disparities, 2022).
- School exclusion: it is estimated that almost all children who are excluded from school have some form of mental health condition (Gill et al., 2017).
What are the largest inequalities in children and young people’s mental health?
An analysis of inequalities in the two contact access rate (the number of children and young people who have received at least two contacts with a mental health service, following a referral) in 2020/21 showed that that greatest inequalities in access to services in Cambridgeshire and Peterborough were by age and ethnicity. Inequalities by deprivation and gender were larger in Cambridgeshire and Peterborough than in other areas in the East of England.
- This graph shows the percentage needed to increase the number of treated children and young people from the group on the left (e.g. boys) to have the same treatment access rate at the group on the right (e.g. girls). The greater the percentage, the larger the inequality.
- Ethnicity is unknown for 13.2% of treated patients; but even if we assume these patients all have a White ethnic background, there would still be an inequality. The grouping of ethnic groups into ‘non-white ethnic minorities’ is likely to have masked underlying differences within this group.
- This analysis was limited as it did not consider other factors that may be linked to inequalities (such as the presence of long-term health conditions) or overlapping experiences of inequalities (such as comparing access rates between boys living in highly deprived areas to girls living in less deprived areas).
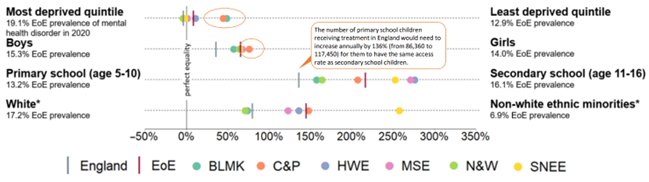
Figure 31: Inequalities in the two contact access rate in the East of England, 2020/21. Image source: Cambridgeshire and Peterborough Children and Young Persons Mental Health ICS Data Insight Pack (June 2022). Note: EoE is the average for the East of England; BLMK is Bedfordshire, Luton and Milton Keynes Integrated Care System (ICS); C&P is Cambridgeshire and Peterborough ICS; HWE is Hertfordshire and West Essex ICS; MSE is Mid and South Essex ICS; N&W is Norfolk and Waveney ICS; and SNEE is Suffolk & North East Essex ICS.
Wider research tells us that:
- The strongest risk factors for depression in young people are a family history of depression and psychosocial stress (with chronic severe stresses, such as negative family relationships and bullying, being the most impactful) (Thapar et al., 2012).
- Children and young people who were female, in their teenage years, or had neurodiverse or chronic physical health conditions were more likely to experience poor mental health in the first year of the COVID-19 pandemic (Samji et al., 2022b).
What are the risk factors for suicide?
‘The death of a child by suicide is an unimaginable tragedy. A young life is lost, a family is devastated, the society where it happens is diminished. The risk, it should be stressed, is low but the need to improve prevention could not be higher.’ – National Child Mortality Database (National Child Mortality Database, 2021)
The National Children Mortality Database analyses child deaths by suicide. The most recent report analysed the 108 probable suicides of children and young people (under 17s) between April 2019 and March 2020, which accounts for around 2 deaths per week (National Child Mortality Database, 2021). Suicides were more common in boys than girls, and 78% of deaths occurred in 15- to 17-year-olds (National Child Mortality Database, 2021). Common risk factors included factors relating to household functioning (such as parental separation and domestic abuse), loss of key relationships and mental health needs (National Child Mortality Database, 2021).
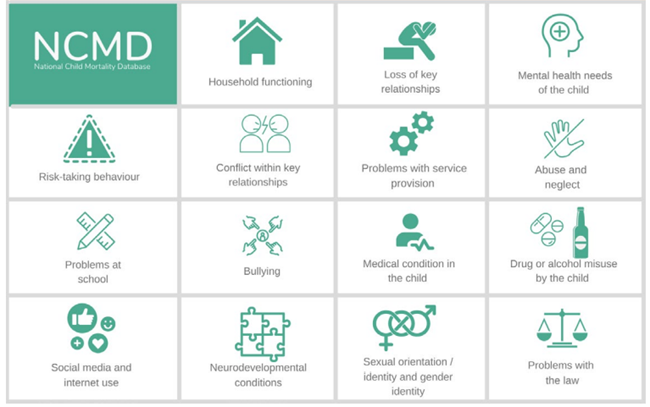
Figure 32: Factors present in suicides, as identified in child death reviews in England from April 2019 to March 2020. Image source: National Child Mortality Database
More recent data shows that deaths by suicide in children and young people did not increase during the first stage of the COVID-19 pandemic (April to December 2020) (Odd et al., 2021).
Additional resources
- Vulnerability in childhood: a public health informed approach
- Tackling mental health disparities: Ten evidence-based actions that government could take in the forthcoming white paper
- Reducing health inequalities faced by children and young people
- Making a Difference to Young People’s Lives through Personalised Care: Mental Health Inequalities and Social Deprivation
- The importance of ethnicity for understanding young people’s experiences of health inequalities
- Young Person’s Toolkit
- Language matters: How to talk about health inequalities in the context of young people
- Inequities in children and young people’s mental health services | The Strategy Unit
- No child left behind: Understanding and quantifying vulnerability
- National Institute of Health Research’s framework for public mental health
- One Call Away, suicide support line for GRT communities: 0774 8997617
- Friends, Families and Travellers: https://www.gypsy-traveller.org/
- One Voice for Travellers: https://onevoice4travellers.co.uk/
- ACERT: https://acert.org.uk/
- The Traveller Movement: https://travellermovement.org.uk/
References
Full list of references is included at the end of this chapter.