Language
Linguistic diversity is increasing across all districts in Cambridgeshire and Peterborough, with more people having a main language other than English in 2021 compared to 2011 (BI Team, 2023). Most people who do not have English as a main language can speak English ‘well’ or ‘very well’.
However, 4.5% of people in Peterborough cannot speak English well or at all; and in Cambridgeshire, 1.2% of people cannot speak English well or at all, ranging from 0.6% in South Cambridgeshire to 2.5% in Fenland (BI Team, 2023). This is means that around 9,400 people in Peterborough and 8,200 people in Cambridgeshire cannot speak English well or at all.
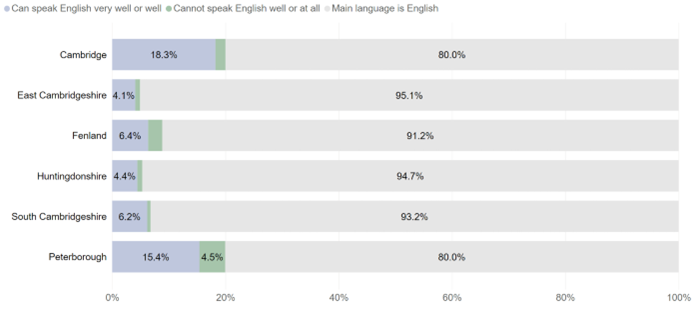
Figure: English language proficiency, Cambridgeshire and Peterborough, Census 2021. Image source: Census 2021 topic summary: ethnic group, national identity, language and religion.
Access
Language barriers and lack of access to interpreter services can prevent people from accessing mental healthcare (Kapadia et al., 2022; Memon et al., 2016). Qualitative research highlights that these barriers can occur across all stages of healthcare, ranging from registering with a GP, to accessing urgent care and understanding diagnoses (Healthwatch, 2022). This can exacerbate health inequalities, particularly amongst people seeking asylum and refugees, who are more likely to experience poor mental health.
Experience
The use of professional translators can minimise language barriers to healthcare (Al Shamsi et al., 2020). Local data shows that different types of translation services are used within Cambridgeshire and Peterborough NHS Foundation Trust (CPFT), with most sessions taking place face-to-face (42%) or by video (39%). A smaller proportion are delivered over the telephone (19%). We do not currently have a good understanding of how translation services are used in relation to need.
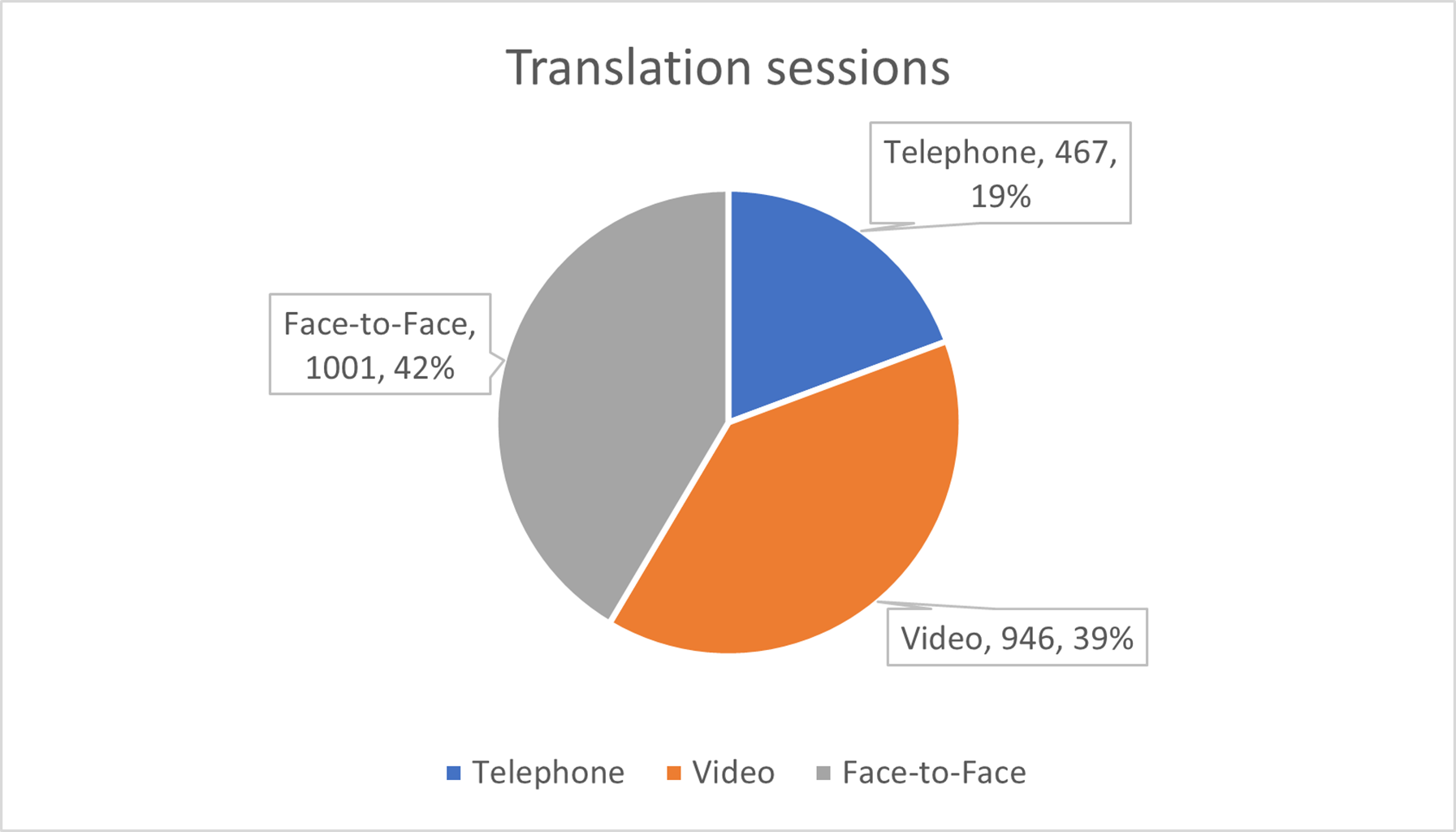
Figure: Method of translation services used in CPFT, August 2022 to September 2023.
The case study below gives an example of a local person’s experience with telephone translation services and how this can pose barriers to accessing healthcare:
” I would like to share my experience about the telephone translation service and its quality. I strongly believe that in certain situations it is better to have an opportunity to use the telephone translation service, instead of not having the conversation at all, however, face to face translation is always incomparably better. I am a person, who had an opportunity to be on both sides – a client, using telephone translation service, and an interpreter, translating on the phone.
As an interpreter, I find it difficult to translate, when I cannot see the person I am translating for. First problem – very often there are network, signal failures and obstructions, when you cannot be sure if the person could hear everything, also, the person cannot tell you this, as they do not know if they missed anything. I personally keep asking during the conversation, if they definitely understand everything I said in their native language. These conversations always last longer than the face to face ones. Quite often there are complete disconnects of the calls and if it is, for example, a jobcentre, the consultant has no right to call the interpreter one more time, so the meeting with the client has to be rearranged.
It is much easier if you can see the person’s face, reactions and emotions so you can make sure the person clearly understands what you tell them. It can be vital, if the conversation is related to serious things like health and wellbeing, domestic abuse, loss, social life. The quality of the translation is very often poor (definitely not always!). I know it, because I help a lot of members of my community and I am next to them when they have phone conversations where the interpreters are involved.
As a client (when I arrived in the UK and could not speak proper English, as well as to understand it well) I found it difficult to share my problem with more and more people. I knew I had to, because the translation service is there for me, to help me, but it was causing anxiety and I tried to avoid it as much as possible. There were certain things I struggled to talk about, because I was thinking, what if the person, who is translating, knows me? If that was a face to face appointment, I would have an opportunity to make sure this is someone who doesn’t not know me or if they do, I would ask for another interpreter (there is that right).
My very recent personal experience when I had the call with the doctor is not positive either. I did not ask for an interpreter, however the lady on the phone, who was speaking my language (Lithuanian), but did not introduce herself, said she would be translating for me. I was surprised, but thanked her and started talking in my language. After 3 minutes of the conversation I said that it would be better if I speak English by myself and it was because she was picking just some certain things from what I said and translating only them to a doctor. I found it not to be useful. After I started speaking English myself, the call was disconnected and the doctor had to call me again.
I know the interpreters and translators are getting paid not enough, so services must use not really skilled people for it. My English was very limited, when I started working for one particular translation agency and was going to the GPs, hospitals, home visits with the social workers to translate, but because they were face to face translations, I could make sure, the person did understand everything.
Even though I was trained to translate on the phone (which, it is believed, is easier and does not include the travel cost, as it is not covered under the employment agreement), I very often refuse to do this, especially for people I do not know.”
Outcomes
Further research is required to build the local and national picture of mental health outcomes for people who do not speak English.
Additional resources
- Lost for words: Healthwatch Evidence on how language barriers contribute to health inequalities
- Language interpreting and translation: migrant health guide
- NHS Accessible Information Standard
References
Full list of references is included at the end of this chapter.