Ethnic minority families
Women from ethnic minority backgrounds are more likely to experience common mental health conditions during the perinatal period (44). For example, compared to White British women, women from Indian and Pakistani ethnic backgrounds are twice as likely to report high levels of psychological distress (44).
Local population
In Cambridge University Hospitals (CUH), at least 19% of births in 2022 were from women from ethnic minority backgrounds, predominantly ‘Asian or Asian British’ ethnicity (10%). In North West Anglia NHS Foundation Trust (NWAFT), at least 21% of births were from women from ethnic minority backgrounds, predominantly ‘Asian or Asian British’ ethnicity (11%) or ‘Black or Black British’ (5%).
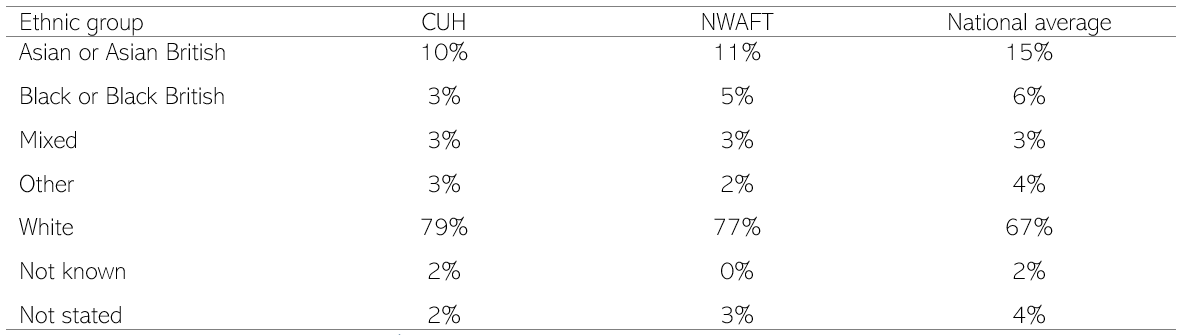
Table 9: Proportion of births by ethnic category of the mother, in December 2022. Data source: National Maternity Dashboard
Note that totals may not add up to 100% due to rounding.
Risk factors for poor mental health
People from ethnic minority groups are more likely to experience a range of risk factors for poor maternity outcomes, as listed in chapter 2 of the needs assessment. Specific risk factors relating to the perinatal period include:
- ‘A ‘one size fits all’ approach to maternity care which does not consider differences in women’s abilities to understand or access care, or serve the most vulnerable appropriately, can result inequalities in healthcare provision, contributing to structural racism’ (60).
- Complications during pregnancy: compared to White ethnic groups, those from Black ethnic groups have higher rates of major postpartum haemorrhage; and those from South Asian and Black ethnic groups are more likely to have their babies admitted to neonatal units (61).
- Preterm births: local preterm birth rates (births before 37 weeks) among mothers from Black ethnic backgrounds are 3.4 times higher in NWAFT, and 2.3 times higher in CUH, than those from White British backgrounds. Mothers with ‘Asian (Indian/Pakistani/Bangladeshi)’ backgrounds have 3 times the rate of preterm births, and White Other around 2.2 to 2.6 times higher, than White British groups (62).
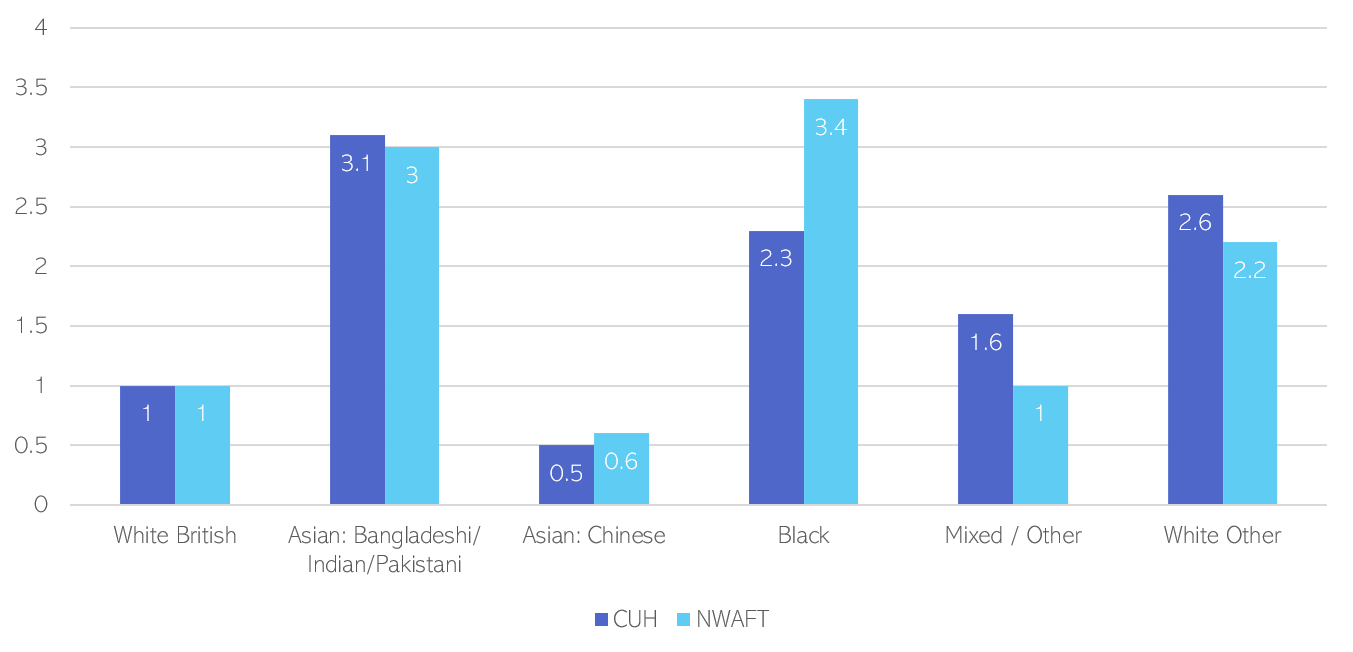
Figure 10: Relative rates of preterm births within ethnicity population (per 100,000) across Cambridgeshire and Peterborough, compared to White British groups, 2020/21. Data source: (62).
Note: the rate of preterm births in White British groups was 23 and 22 per 100,000 of the ethnicity population, in CUH and NWAFT respectively.
Access
National research suggests that:
- Women from ethnic minority backgrounds are less likely to be asked about their mental health during pregnancy and the postnatal period, to be offered treatment and to receive support (52).
- Compared to White British women, women from Black African, Asian and ‘White Other’ ethnic groups are less likely to access community mental health services, and more likely experience involuntary admission to mental health services during the perinatal period (63).
- Women from these groups have a higher number of attended community contacts, and fewer non-attendance or cancelled appointments, which suggests there are inequalities in access to services rather than differences in engagement (63).
- Compared to White British women, Indian women are half as likely, and Black African women are a third as likely, to receive treatment for postnatal depression or anxiety (44).
- Gypsy and Travellers may not gain full access to maternity services and some may experience poor continuity of care, such as when forced to suddenly move from a site (64).
Reviews suggests that women from ethnic minority backgrounds may face additional barriers to accessing support services for perinatal mental health problems (43). Many of these were covered in chapter 2 of this needs assessment. International studies also suggest that women from non-Western cultures may be more likely to report somatic symptoms of perinatal mental health conditions, which are not recognised in most screening tests used in the NHS (65).
The NHS has pledged to improve equity in maternity services and race equality for NHS staff (38), which has led to the development of Cambridgeshire and Peterborough Better Births Equality and Equity Plan
Experience
- The maternity experiences of local families from ethnic minority backgrounds have been collected by the Raham Project. This organisation anonymously informs the local maternity services about the experiences they hear and works with them to change the way care is delivered. Key themes in their 2022 annual report include:
- Many women had positive experiences of birth. However, difficult birthing experiences could have a long-term impact on mental health. Some women experienced disrespectful, discriminatory and stereotyping attitudes from healthcare professionals and did not feel involved in decision making.
- Some women benefited from supportive relationships with midwives, but it could be difficult to establish this without consistency of care.
- Some women felt that their family situation impacted their mental health. Many highlighted the importance of support for breastfeeding to maintaining good mental health.
- Co-production with Muslim women in Peterborough brought together experiences of multiple women into 3 personas, who highlight common experiences and feelings (66). The story of one of these personas, Amal, is given below:
Amal’s Story (66)
‘Amal has a refugee background. She and her three children had to flee from the dangers of war-torn Syria, her country of birth, leaving her husband behind. Amal and her children had to cross several countries before arriving in England. They subsequently spent six weeks at Yarl’s Wood immigration detention centre in Bedford. The prolonged stay, however, meant that she did gain the right to remain in the UK. She was then sent to Peterborough where there was available temporary accommodation. Alongside this ordeal, Amal was grieving the loss of her brother Carim, who was killed during protests of unrest in Syria. This combined experience of loss, grief, stress and uncertainty had a significant negative impact on Amal’s mental health.
Amal arrived at her temporary accommodation to be faced by a host of challenges that she hadn’t previously considered. She had little understanding of the English language and her ability to speak it was even less, the culture and way of life in the UK was also very different to her home country and she had very little financial support or knowledge as to where to seek help.
Amal feels under enormous pressure, especially given that she has a young baby and two other children under seven years. Her mental health has declined further, not helped by the fact that she suffers flashbacks and nightmares from her time in Syria which are severely affecting her sleep. The housing association responsible for Amal’s temporary accommodation has tried to help by referring her to a psychotherapist however as well as the language barrier, she cannot take her children with her to the appointments, and she has no-one to help with her childcare.
Amal feels isolated and frightened. She is used to receiving support from her husband and wider family but is having to face all of these new challenges alone. This isolation is exacerbated by the fact that Amal doesn’t have a motivation to go out and meet new people. She fears discrimination and racism because she doesn’t speak English and wears a hijab. That said, Amal is very keen to learn English, as she believes this is key to a good life in the UK. She also dreams of getting a job but can’t do so because she has no childcare. The only regular communication that Amal has with others is with her immediate family by phone. She strives to apply for a visa for her husband through family reunification scheme and is putting all her effort into getting everything in place to make this happen.’ – Source: Starting Well-Perinatal Mental Health Support for Muslim Communities Insight Report.
- A review of ethnic minority women’s experiences of maternity services in the UK found that (67):
- Care was often perceived as ‘functional’ rather than supportive.
- Some women experienced prejudice or discrimination based on their ethnicity, religion or culture.
- Several women reported communication failures, including language barriers and inadequate signposting when navigating complex systems.
- Where resources allowed, there were reports of women-centred care, which was non-judgemental, and provided continuity of carer and cultural safety.
- A review of Muslim women’s experience of maternity services in the UK highlighted that (68):
- The majority of women experienced poor maternity care, which was sometimes the result of discriminatory behaviour.
- Communication issues, lack of interpreters and inadequate access to appropriate information were key concerns. Many women also felt there was a lack of understanding and awareness of their decision making processes and how these related to Islamic practices.
- National research has found that Gypsy, Roma and Traveller communities face barriers to accessing and maintaining continuity of care, discrimination within healthcare and other public services, and a lack of accessible information in maternity services (187).
Existing policy interventions designed to tackle ethnic health inequalities in maternal and neonatal health were reviewed in 2022. This report identified the following actions for integrated care system leaders and voluntary and community sector groups:
- Evaluations of local interventions should be built into their design. Targets for interventions should be realistic and measurable.
- Family Hubs should provide population health-based interventions to improve pre-conception health and provide a platform that links up local maternity systems and integrated care systems, to meet the specific needs of target populations.
Voluntary and community sector groups should co-produce interventions and research with women from ethnic minority groups, in particular Black African and Black Caribbean, Roma and Gypsy ethnic groups.
Additional resources
- Maternity high impact area: Reducing the inequality of outcomes for women from Black, Asian and Minority Ethnic (BAME) communities and their babies
- Perinatal Mental Health of Black and Minority Ethnic Women: A Review of Current Provision in England, Scotland and Wales
- The Black Maternity Experiences Report
- Starting Well – Perinatal Mental Health Support for Muslim Communities captures the experiences of Muslim mums in Peterborough
- Embedding cultural awareness in maternity services
- Improving the way family support services work for minority ethnic families
- Guidance: Tackling Maternal Health Inequalities in Gypsy, Roma and Traveller Communities
References
43. Watson H, Harrop D, Walton E, Young A, Soltani H. A systematic review of ethnic minority women’s experiences of perinatal mental health conditions and services in Europe. PLoS One. 2019;14(1).
44. Moore L, Jayaweera H, Redshaw M, Quigley M. Migration, ethnicity and mental health: evidence from mothers participating in the Millennium Cohort Study. Public Health. 2019;171.
52. Redshaw M, Henderson J. Who is actually asked about their mental health in pregnancy and the postnatal period? Findings from a national survey. BMC Psychiatry. 2016;16(1).
60. Public Health England. Maternity high impact area: Reducing the inequality of outcomes for women from Black, Asian and Minority Ethnic (BAME) communities and their babies [Internet]. 2020 [cited 2023 Mar 27]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/942480/Maternity_high_impact_area_6_Reducing_the_inequality_of_outcomes_for_women_from_Black__Asian_and_Minority_Ethnic__BAME__communities_and_their_babies.pdf
61. Royal College of Obstetricians and Gynaecologists. National Maternity and Perinatal Audit: Ethnic and Socio-economic Inequalities in NHS Maternity and Perinatal Care for Women and their Babies [Internet]. 2021 [cited 2023 Mar 7]. Available from: https://maternityaudit.org.uk/FilesUploaded/Ref%20308%20Inequalities%20Sprint%20Audit%20Report%202021_FINAL.pdf
62. Philips L. Cambridgeshire and Peterborough Local Maternity & Neonatal System Equity and Equality Analysis [Internet]. 2022 [cited 2023 Mar 10]. Available from: https://www.cpics.org.uk/children-and-maternity
63. Jankovic J, Parsons J, Jovanović N, Berrisford G, Copello A, Fazil Q, et al. Differences in access and utilisation of mental health services in the perinatal period for women from ethnic minorities – A population-based study. BMC Med. 2020;18(1).
64. Matthews Z. Better Health Briefing: The health of Gypsies and Travellers in the UK [Internet]. 2008 [cited 2023 Feb 15]. Available from: https://www.gypsy-traveller.org/wp-content/uploads/health-brief.pdf
65. Womersley K, Ripullone K, Hirst JE. Tackling inequality in maternal health: Beyond the postpartum. Future Healthc J. 2021 Mar;8(1):31–5.
66. CPSL Mind. Starting Well-Perinatal Mental Health Support for Muslim Communities Insight Report [Internet]. 2021 [cited 2023 Feb 28]. Available from: https://static1.squarespace.com/static/5d6801ff19efcd000178e7e5/t/63beb2ae613b264b86add7ff/1673441995973/TLI_Perinatal_Report.pdf
67. MacLellan J, Collins S, Myatt M, Pope C, Knighton W, Rai T. Black, Asian and minority ethnic women’s experiences of maternity services in the UK: A qualitative evidence synthesis. J Adv Nurs. 2022;78(7).
68. Firdous T, Darwin Z, Hassan SM. Muslim women’s experiences of maternity services in the UK: Qualitative systematic review and thematic synthesis. BMC Pregnancy Childbirth. 2020;20(1).
69. Esan OB, Adjei NK, Saberian S, Christianson L, Mchale P, Pennington A, et al. Mapping existing policy interventions to tackle ethnic health inequalities in maternal and neonatal health in England: A systematic scoping review with stakeholder engagement [Internet]. 2022 [cited 2023 Apr 24]. Available from: https://www.nhsrho.org/wp-content/uploads/2022/12/RHO-Mapping-existing-policy-interventions_December-2022.pdf