Physical health and severe mental illness
‘People with severe mental illness have a reduced life expectancy of 15–20 years, yet the majority of reasons for this are avoidable. This can no longer be tolerated in the 21st century’ (Royal College of Psychiatrists, 2013)
People living with severe mental illness (SMI) face substantial inequalities in health. Severe mental illnesses are mental health conditions which severely limit people’s ability to engage with work and other activities (National Mental Health Intelligence Network, 2018). They are typically long lasting and may involve hospitalisation or psychosis. Developing a physical health condition, particularly those that result in fatigue and reduced mobility, can make it more challenging for people living with severe mental illness them to participate in education, employment, or looking after their families (Doherty & Gaughran, 2014). This can increase their risk of social isolation, which can have exacerbate poor mental health.
Why do people with severe mental illness face physical health inequalities?
Factors contributing to this gap in life expectancy include barriers to healthcare factors, patient factors and wider system factors side effects of antipsychotic medication, and health behaviours (Reilly et al., 2015).
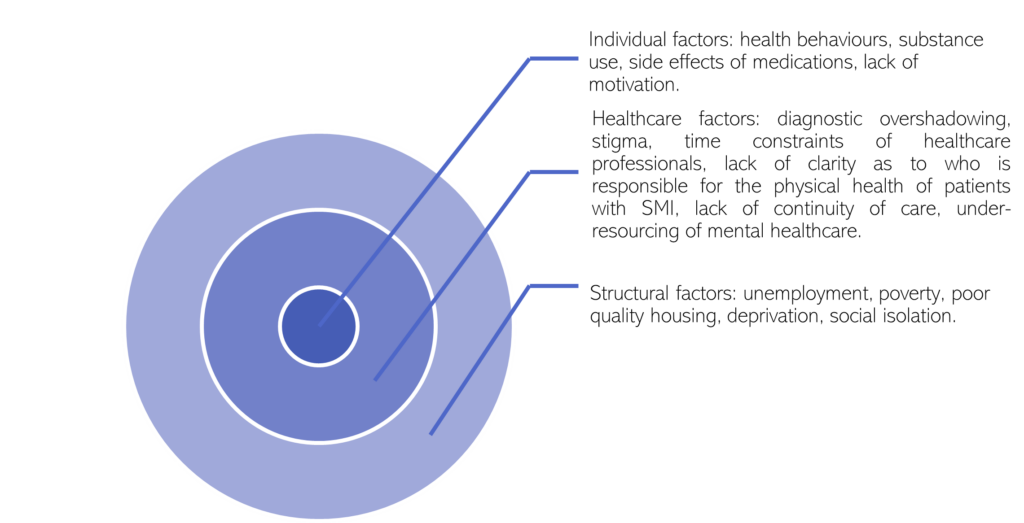
Figure 108: Interrelated factors contributing to physical health inequalities in people with severe mental illness. Adapted from: (Lawrence & Kisely, 2010)
Structural factors
- People with severe mental illnesses are more likely to experience socioeconomic factors that can lead to poor physical health, such as unemployment, poverty and poor-quality housing (Davies, 2016).
- See more about why employment is important to mental health.
Healthcare factors
- Most people with severe mental illnesses do not receive adequate physical healthcare (J. Firth et al., 2019). For example, people with SMI are less likely to receive preventative healthcare (such as cancer screenings) or health promotion interventions (such as support with smoking cessation) (Naylor et al., 2016).
- People with severe mental illnesses may experience diagnostic overshadowing, whereby their physical symptoms are incorrectly attributed to their mental health condition (Naylor et al., 2016).
- People with mental health conditions are less likely to receive the correct prescription for physical health conditions (A. J. Mitchell et al., 2012).
- People with severe mental illnesses often experience poor continuity of care (Reilly et al., 2012), despite research showing that patients believe it is important for them to consistently see the same GP (Lester et al., 2005).
Individual factors
- Many psychiatric medications, especially antipsychotics, are associated with an increased risk of high blood pressure and raised blood pressure (de Hert et al., 2012).
- Symptoms of mental health conditions may impact people’s ability to seek appropriate healthcare interventions or advocate for themselves (Davies, 2016). For example, patients with severe mental illness who have health problems are less likely to report them to their GP, due to self-neglect, impaired motivation and social withdrawal (Ride et al., 2018).
What is the national picture?
Morbidity
People with severe mental illness are more likely than those in the general population to have a range of physical health conditions, including being 1.9 times more likely to have diabetes and 2.1 times more likely to have chronic obstructive pulmonary disease (Public Health England, 2018b).
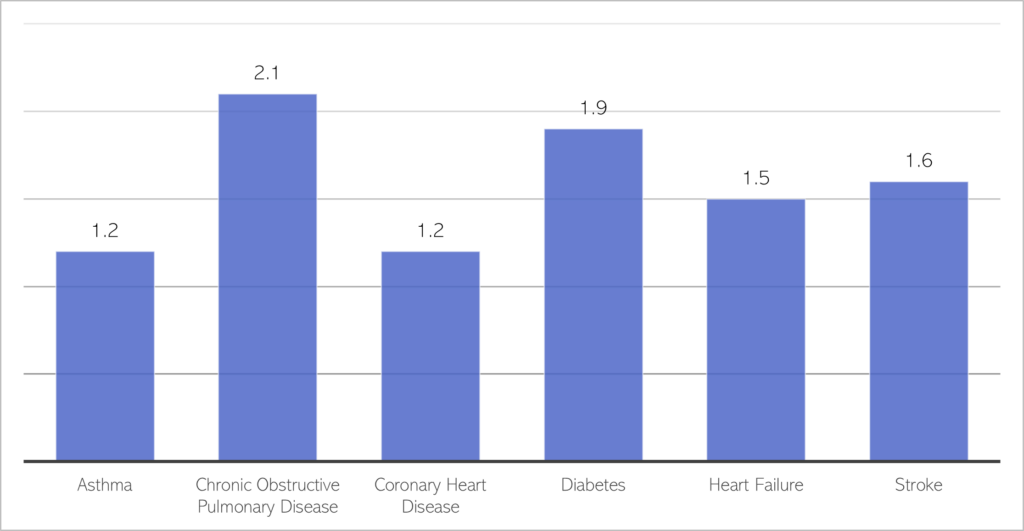
Figure 103: When compared to other 15 to 74 year olds in the general population, how many more times likely are people with SMI to have the following long-term health conditions? Data source: (Public Health England, 2018b)
- Health inequalities are even more extreme for younger adults with severe mental illness (aged between 15 and 34) who, compared to their peers, are (Public Health England, 2018b):
- 3 times more likely to obese.
- 1.3 times more likely to have asthma.
- 3.7 times more likely to have diabetes.
- 3.2 times more likely to have hypertension.
- People with servere mental illness are also more substantially more likely to experience chronic pain: for example, 1 in 4 (24%) people with bipolar live with chronic pain and 1 in 7 (14%) experience migraines, which is over twice and 3 times the rates in the general population (Stubbs et al., 2015).
- People with severe mental illness are more likely to experience physical multimorbidity, including being 1.8 times more likely than the general population to have two or more physical health conditions (Public Health England, 2018c).
- Whilst co-morbidity refers to having at least one physical health condition alongside a mental health condition, multimorbidity is being used here to describe having multiple physical health conditions and a SMI.
- Young people (aged between 15 and 34) with severe mental illness are 5 times more likely to have 3+ physical health conditions than their peers (Public Health England, 2018b).
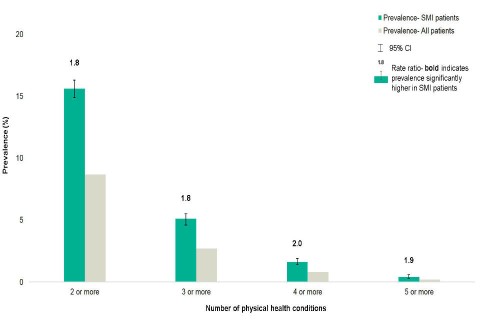
Figure 104: Prevalence of physical health multi-morbidities for people with SMI aged between 15 to 74. Source: Public Health England
- Co-morbidity rates for people with severe mental illness vary by ethnicity. For example, compared to White British people with psychosis (Fonseca De Freitas et al., 2022):
- Black African, Black Caribbean and Black British people with psychosis are 1.5 times more likely to have at least one physical health condition; whereas Chinese people or those from ‘other’ ethnic groups are less likely to have a physical health condition.
- Black African, Black Caribbean and Black British people with psychosis are around 2 times as likely to have 3 physical health conditions.
- People with severe mental illness living in highly deprived areas are more likely to experience physical health conditions such as asthma, diabetes and chronic obstructive pulmonary disorder; as well as to experience multiple physical health conditions (Public Health England, 2018c).
- People with severe mental illness are more likely than the general population to access emergency care, which may suggest that primary care is not meeting the physical health needs of this group. For example, compared to the general population, people with SMI are (NHS England, 2017a):
- 3 times more likely to attend A&E with an urgent physical health need.
- Almost 5 times more likely to have an emergency hospital admission.
- Rates of COVID-19 vaccination uptake are lower in people with severe mental illness than other people in the same vaccine priority group (Arumuham et al., 2022).
Mortality
People with severe mental illness die on average 15 to 20 years earlier than the general population (Chesney et al., 2014), and the gap between the life expectancy of people with severe mental illness and the general population in the UK is increasing (Hayes et al., 2017).
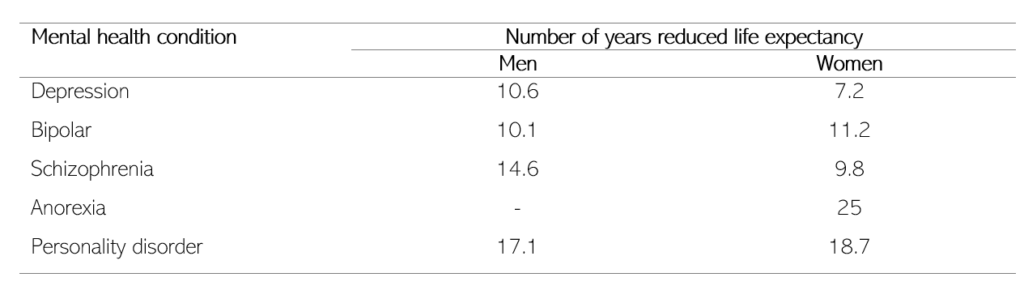
Table 36: Number of years of life expectancy for people with different mental health conditions. Data source: (Byrne, 2022)
It has been estimated that 2 in every 3 deaths of people with severe mental illness could be prevented (Public Health England, 2018c). People with schizophrenia die on average 28.5 years earlier than adults in the general population, with 85% of the deaths being attributable to natural causes, including cardiovascular disease (35%), cancer (17%) and diabetes (5%) (Olfson et al., 2015).
Compared to the general population, people with severe mental illness are several times more likely to die from a variety of causes, including suicide, cardiovascular disease and cancers (Das-Munshi et al., 2017).
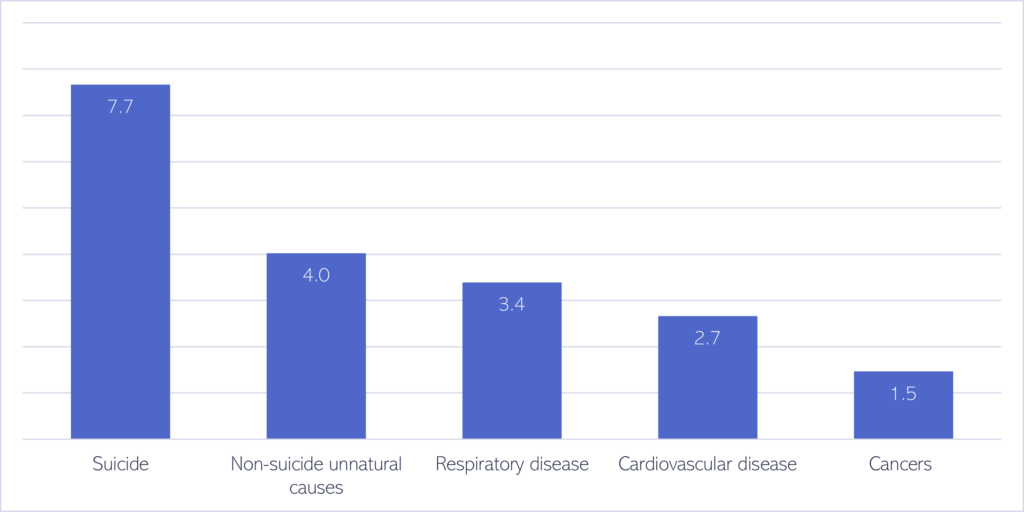
Figure 105: How more times likely are people with SMI to die from the following causes, compared to the general population. ‘Unnatural causes’ of death include any deaths not due to natural causes, such as accidents, overdoses and falls. Data source: (Das-Munshi et al., 2017)
- Among people with severe mental illness, people from Black African, Black Caribbean and South Asian groups have lower mortality rates than people from White British groups (Das-Munshi et al., 2017). The reasons behind this are unclear.
- People with severe mental illness were at a greater risk of death during the first wave of the COVID-19 pandemic, both from COVID-19-related and other causes. For example, compared the general population, the risk of death from COVID-19 in the first quarter of 2020 was (Das-Munshi et al., 2021):
- 3.3 times higher for people with schizophrenia.
- 4.8 times higher for people with eating disorders.
- 4.6 times higher for people with personality disorders.
Annual physical health checks
- To address the extreme inequalities faced by people with severe mental illness, the NHS Long Term plan proposed that greater numbers of people with severe mental illness should receive annual physical health checks (NHS, 2019).
- People with severe mental illness from Black African and Caribbean ethnic groups report (Phillips, 2022):
- Varying levels of awareness of primary care health checks, depending on locality.
- A lack of engagement from healthcare professionals as to why health checks are important.
- Experiencing barriers to uptake, including difficulties making GP appointments, substance use and stigma around accessing primary care. People also reported being apprehensive about using services due to fears around being sectioned and perceptions that staff lacked cultural awareness.
- There is some evidence to suggest that carrying out physical health checks, without further follow up or intervention, may not be enough to improve the healthcare or health outcomes of patients with severe mental illness.
- For example, a national evaluation of primary care incentives promoting physical health checks found improvements in the identification of cardiovascular risk factors, but not the pharmacological management of these risks (C. L. Wilson et al., 2017).
- There is no association between attendance at annual health checks and risk of presenting to A&E or of being admitted to hospital (Ride et al., 2018).
What is the local picture?
- Rates of premature mortality for people with severe mental illness are significantly worse than the national average in Peterborough for both men and women; though for men in Cambridgeshire, rates are below average.
- Note that adults with referrals to secondary mental health services is used as a proxy for severe mental illness. This omits patients with severe mental illness who only have contact with primary care; and includes patients with referrals to secondary mental health services for common mental health disorders.
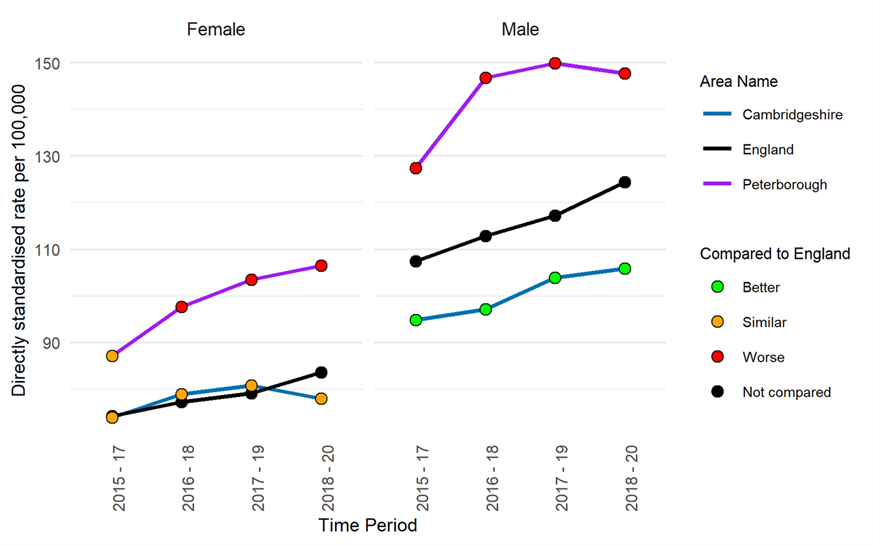
Figure 106: Premature mortality in adults with SMI. Data source: (Office for Health Improvement and Disparities, 2022b)
- Excess premature mortality rates for people with severe mental illness show an overall increasing trend for both men and women in Cambridgeshire and Peterborough since 2015.
- The most recent figures for Cambridgeshire show that the risk of dying prematurely for people with severe mental illness was 515.7% higher for women and 496.3% higher for men, compared to those who do not have severe mental illness. This is significantly higher than the national averages.
- In Peterborough, the risk of dying prematurely for those with severe mental illness was 378.7% higher for women and 357.3% higher for men, than those who do not have severe mental illness. This is statistically similar to the national averages.
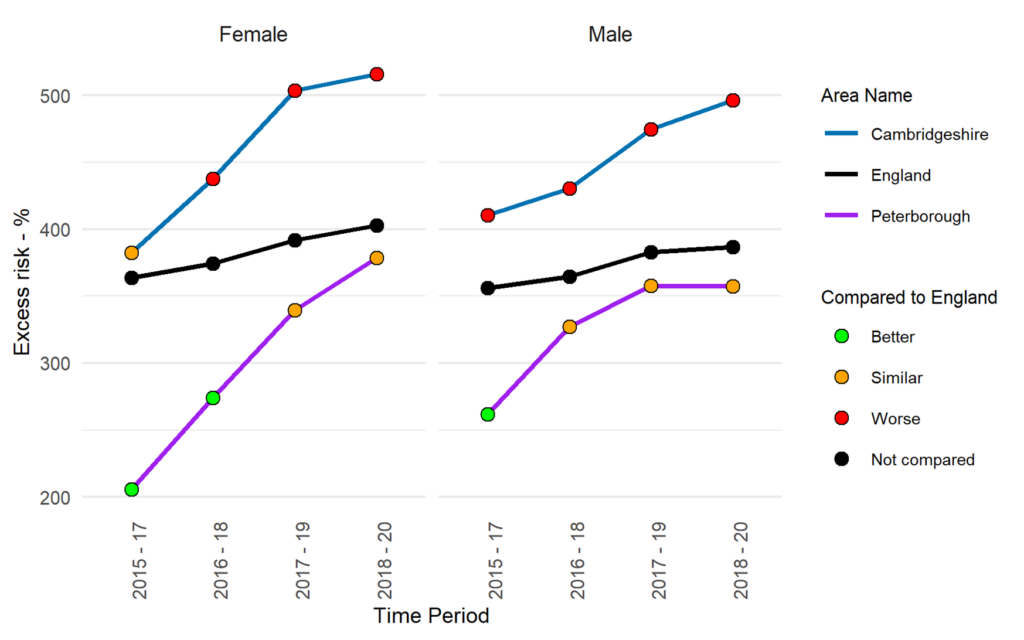
Figure 107: Excess under 75 mortality rate in adults with severe mental illness: Data source: (Office for Health Improvement and Disparities, 2022b)
Premature mortality and excess under 75 mortality rates due to specific conditions (cardiovascular disease, cancer, respiratory disease, and liver disease) can be found here.
Additional resources
- The local data pack gives an overview of key data and trends
- Equally Well UK, a collaborative supporting the physical health of people with a mental illness
- Closing the Gap: Inequalities and severe mental ill health
- NIHR summary of how physical health is important to public mental health
- Public Health England briefing on Severe mental illness (SMI) and physical health inequalities
- Improving the physical health of adults with severe mental illness: essential actions
- Physical health and severe mental illness scenario Tom’s journey: An implementation support resource that highlights the variation between optimal and suboptimal pathways
- HEAT Core20PLUS5 Toolkit: this toolkit contains an adapted version of the HEAT tool for severe mental illness
References
Full list of references is included at the end of this chapter.