Physical health and common mental health conditions

Figure 97: A summary of the links between poor physical health and common mental health conditions. Data sources: [(NHS England & NHS Improvement, 2018a), (Naylor et al., 2012), (Naylor et al., 2016), (Gureje et al., 1998)]
People with poor physical health are more likely to develop mental health conditions
- 30% of people with long-term physical health conditions also have a mental health condition (NHS England & NHS Improvement, 2018a), which is 2 to 3 times the prevalence in the general population (Naylor et al., 2012).
- Children with physical health conditions are almost twice as likely to have a mental health condition than those in good physical health (Parry-Langdon & Great Britain. Office for National Statistics., 2008).
- 2 in 3 hospital beds are occupied by older people, up to 60% of whom have or develop a mental health problem during their admission (Naylor et al., 2016). The close relationship between the physical and mental health of older people was explored the Older People’s Health Needs Assessment (Cambridgeshire County Council, 2014).
- Depression and anxiety are the most common types of co-morbid mental health conditions (NHS England & NHS Improvement, 2018a).
- Over 40% of outpatients with medically unexplained symptoms (physical symptoms that lack an identifiable organic cause) also have anxiety or depression (Naylor et al., 2016). Medically unexplained symptoms will be covered in more detail in the chapter on working-age adults.
- Some physical health conditions have particularly strong links with poor mental health. For example, compared to those who do not experience chronic pain, people who report chronic pain for a period of at least 6 months are 4 times more likely to have anxiety and 1.6 times more likely to have significant limitations on their daily activity (Gureje et al., 1998).
- Similarly, people with multiple physical health conditions (multimorbidity) are more likely to have poor mental health (Naylor et al., 2012):
- People with 3 or more health conditions have a significantly poorer quality of life and lower levels of physical functioning than those with 1 or 2 conditions (J. S. Williams & Egede, 2016).
- Within those who have multiple health conditions, people with chronic pain, reduced mobility or who are socially isolated are more likely to have co-morbid mental health conditions (Taskforce on Multiple Conditions, 2018).
- Polypharmacy, the concurrent use of multiple medications, can increase the risk of adverse side effects from drugs and drug interactions. This can have a negative impact on people’s quality of life (Duerden et al., 2013).
Having a mental health condition increases your risk of poor physical health
- 46% of people with a mental health condition have a long-term physical health condition (Naylor et al., 2012).
- Mental health conditions are associated with an increased risk of poor physical health. For example, having depression is associated with a (Royal College of Psychiatrists, 2013):
- 50% increased risk of dying from any disease.
- 2 times increased risk of having coronary heart disease or diabetes.
- 3 times increased risk of dying in the next 4 years.
- Having a mental health condition is also associated with an increased risk of physical health multimorbidity:
- People with common mental health conditions, SMI and substance use are at all a greater risk of physical multimorbidity, from illness onset (J. Firth et al., 2019).
- People with mental health conditions develop physical health multimorbidity at a younger age than those in the general population (J. Firth et al., 2019).
- People with both physical and mental health conditions (co-morbidity) have poorer health outcomes and a worse quality of life than those without co-morbidity (Naylor et al., 2012).
- People with mental health conditions have higher rates of emergency hospital use for physical health problems, including 3.6 times the rate of potentially avoidable emergency admissions (Naylor et al., 2016).
- People in contact with specialist mental health services have 3.6 times the morality rate of the general population (NHS Digital, 2013).
- Specific combinations of physical and mental health conditions are associated with much higher levels of healthcare use and mortality (Zhu et al., 2020):
- For under 65s, the combination of depression, anxiety and pain is associated with the greatest level of contact with GPs.
- In 65- to 85-year-olds, people who experience chronic pain, coronary heart disease and depression have the highest mortality rate and greatest level of health service use (contact with GPs, hospitalisations and repeat prescriptions).
Why is there a link between physical and mental health?
The relationship between mental and physical health is bidirectional (Naylor et al., 2012), and is influenced by common social determinants of health, including poverty, social isolation and discrimination.
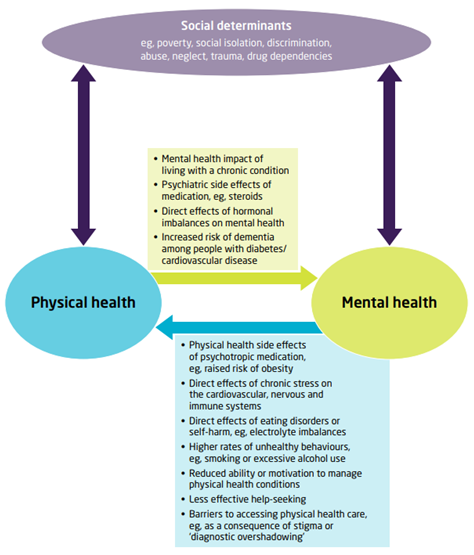
Figure 98: The interactions between physical and mental health. Source: King’s Fund
Mental health conditions can contribute to and exacerbate poor physical health
- Some mental health conditions have direct physical impacts, such as the long-term effects of eating disorders (O’Brien et al., 2017).
- Medications used to treat mental health conditions can increase the risk of poor physical health (J. Firth et al., 2019).
- People with mental health conditions may experience diagnostic overshadowing, which is when symptoms of physical illness are wrongly attributed to a mental health condition. This can arise from a range of reasons, including stigma around mental health (S. Jones et al., 2008).
- Some people with mental health conditions may be less likely to seek help for physical health symptoms (Phelan et al., 2001).
- Poor mental health can make it difficult for people to engage in activities that improve their physical health, such as quitting smoking (see Smoking and Health Behaviours).
- Some people with mental health conditions may be less able to adhere to treatment for physical health conditions (Margaretten et al., 2011). For example, people with depression have 3 times the risk of not complying with recommended treatment for a range of physical health conditions, compared to those without depression (DiMatteo et al., 2000).
Poor physical health can negatively impact mental health
- Some physical illnesses and their treatments physiologically impact mental health, such as the link between systematic inflammation and depression (Margaretten et al., 2011).
- Being diagnosed with a long-term physical health condition can lead to a period of profound internal adjustment (Naylor et al., 2016).
- People with long-term health conditions are more likely to experience low self-esteem, stigma and discrimination, and social isolation (NHS England, 2016a).
- Being unable to work due to poor physical health can cause or exacerbate mental health problems (Vo et al., 2015).
Common social determinants of health
- People who have had more adverse childhood experiences report having poorer physical and mental health (Logan-Greene et al., 2014).
- There is a strong association between multimorbidity and levels of household wealth (Singer et al., 2019). People with lower incomes have fewer resources to manage living with long-term health problems.
- Loneliness in older people is associated with poor physical and mental health outcomes, including hypertension, cognitive decline and depression (Luanaigh & Lawlor, 2008).
Example: type 2 diabetes and depression
These links are exemplified by the close relationship between type 2 diabetes and depression:
- 15% to 30% of people with type 2 diabetes have depression, around twice the rate in the general population (Richardson et al., 2005).
- People with depression are more likely to develop type 2 diabetes (Imison, 2021).
- Poor diabetes control often intensifies the symptoms of depression. Likewise, depression can worsen diabetes outcomes, including increasing the risk of morbidity and mortality (Imison, 2021). For example, people with both diabetes and depression have a 36 to 38% greater risk of dying over a 2 year follow up period, compared to those who only have diabetes (Naylor et al., 2012).
- People with poor mental health and type 2 diabetes have more hospital admissions and complications than those with good mental health (NHS England, 2017a).
- This results in a 50% increase in costs for the physical healthcare of type 2 diabetes, resulting in £1.8 billion of additional spending across the NHS each year (NHS England, 2017a).
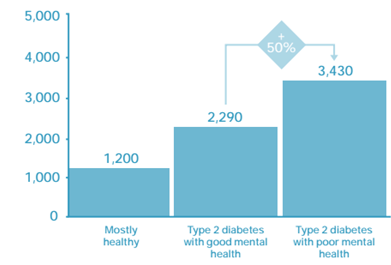
Figure 88: Annual physical healthcare costs (£) of healthy patients, and patients with type 2 diabetes who have good and poor mental health, 2014/15. Note that these calculations do not including spending on psychiatric drugs or other mental health services. Source: NHS England
- Factors contributing to the poorer outcomes faced people with co-morbid diabetes and depression include that some antidepressants influence blood glucose levels (Imison, 2021), and that depression can limit people’s motivation, energy and ability to adhere to diabetes treatment (Imison, 2021).
- Furthermore, an audit of diabetes care in inpatient mental health wards across London found that change was needed to ensure diabetes care was patient-centred (Health Innovation Network, 2022):
- 34% of patients felt they had not been involved in their diabetes care during their stay.
- Almost all trusts lacked access to their own diabetes specialist resource.
What is the national picture?
Across England, there is a substantial overlap between people who have long-term physical health and mental health conditions (Naylor et al., 2012). Long-term physical health conditions are defined here as conditions that can be managed but often not cured, such as diabetes, arthritis and asthma.
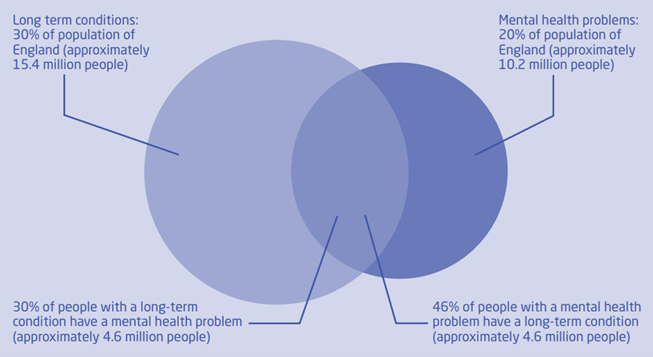
Figure 89: The overlap between long-term physical health conditions and mental health problems in England. Source: King’s Fund
The prevalence of co-morbid mental and physical health conditions increases dramatically by age and deprivation level (Cassell et al., 2018).
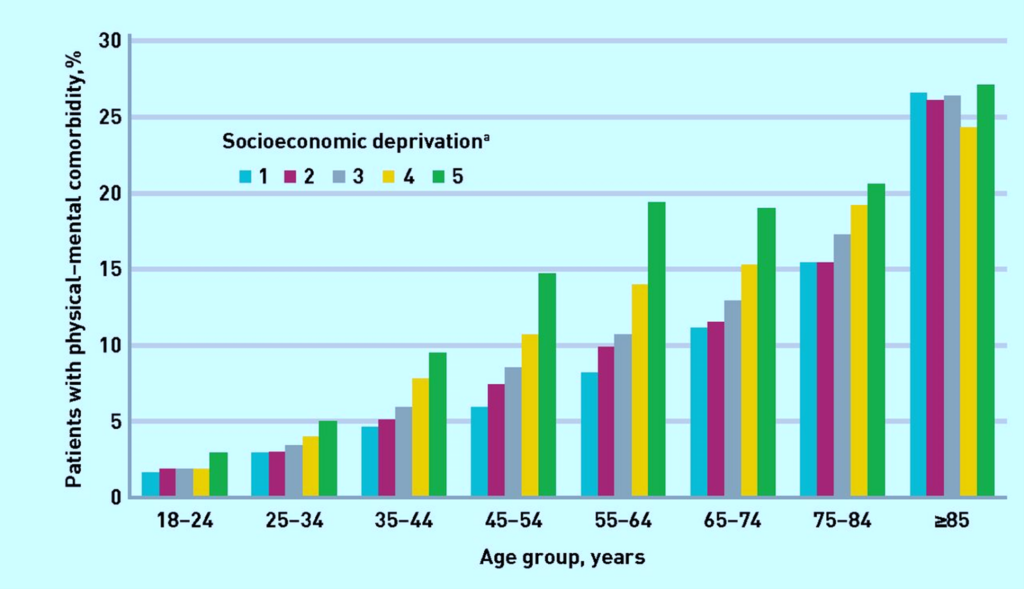
Figure 90: Prevalence of physical–mental comorbidity by age and socioeconomic status. 1 indicates the areas with the lowest, and 5 the highest, levels of deprivation. Source: Cassell et al.
- Being diagnosed with a severe physical illness, such as chronic obstructive pulmonary disease or a degenerative neurological condition, is associated with a 2 to 3 times higher suicide risk in the first year following diagnosis (Nafilyan et al., 2022). The risk of suicide is highest in the first 6 months post-diagnosis.
- Over 7 million people are on NHS waiting lists for elective care, the largest number on record. This is equivalent to 1 in 8 people in England (QualityWatch & The Nuffield Trust, 2022). As long waiting times for operations are associated with depression, anxiety and deteriorating quality of life for patients and caregivers, this is likely to have a significant impact on mental health (Gagliardi et al., 2021).
What is the local picture?
There are over 60,000 people in Cambridgeshire and Peterborough who have both physical and mental health conditions, however the prevalence of comorbidity is not evenly distributed across Cambridgeshire and Peterborough. Fenland and Peterborough have significantly higher rates of co-morbidity than the Cambridgeshire and Peterborough average.
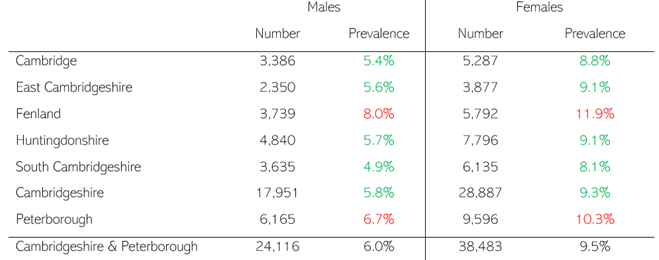
Table 35: Number and prevalence of people with physical and mental health comorbidity by sex in Cambridgeshire and Peterborough, 2011. Red indicates a significantly higher prevalence, and green significantly lower, than the prevalence across Cambridgeshire and Peterborough. Data source: (O’Neill, 2018)
A review of Cambridgeshire and Peterborough NHS services in 2017 found that (The Strategy Unit, 2017):
- The life expectancy of men in contact with mental health services was 63.3 years, 20 years lower than men in the rest of the population.
- The life expectancy of women in contact with mental health services was 70.0 years, 16.2 years lower than women in the rest of the population.
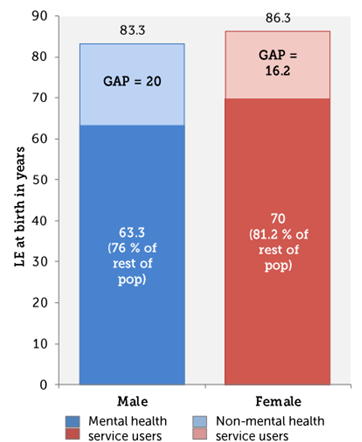
Figure 91: Life expectancy (LE) at birth in people who are and are not in contact with mental health services, from 2012/13 to 2014/15. Source: The Strategy Unit
In 2017 in Cambridgeshire and Peterborough, compared to the rest of the population, (The Strategy Unit, 2017):
- People using mental health services were 3 to 4 times more likely to die from cancers, circulatory disease and respiratory disease.
- People using mental health services were around 3 times more likely to use Accident and Emergency services and to have an emergency admission to hospital.
Premature Mortality

Recent analysis has been conducted looking at premature mortality rates for patients in contact with mental health services – Mental health contacts and premature mortality 2020-2024
Additional resources
- The local data pack gives an overview of key data and trends
- How physical and mental health interact: A basic model
- The Lancet Psychiatry Commission: a blueprint for protecting physical health in people with mental illness
- Equally Well UK, a collaborative supporting the physical health of people with a mental illness
- The King’s Fund reports Long-term conditions and mental health and integrated care
- NHS England’s report Improving the physical health of people with mental health problems: Actions for mental health nurses
- Making the case for integrating mental and physical health care
- Cambridgeshire Insight health report, which includes data on physical health
- The Strategy Unit report Making the case for integrating mental and physical health care for Cambridgeshire and Peterborough
References
Full list of references is included at the end of this chapter.