Barriers to mental health support
Public Health England guidance, published in 2017, highlighted two key principles for services supporting people with co-occurring conditions (Public Health England, 2017): that meeting the needs of this group is ‘everyone’s job’, and that there should be a ‘no wrong door’ approach for people accessing support.
Figure 125: Key principles for services supporting people with co-occurring conditions, as identified in 2017 Public Health England guidance. Adapted from: (Public Health England, 2017)
What is the local picture?
Previous needs assessments (Solutions for Public Health, 2014) highlighted the need for more integrated care to meet both mental health and substance use needs (Public Health England, 2019a). These reports led to local commitments being made in 2020 to provide better care for people with co-occurring conditions (Cambridgeshire and Peterborough CCG et al., 2020), as based on the above Public Health England guidance (Public Health England, 2017).
This commitment covered all professionals working in mental health, substance use and criminal justice, and aims to ensure that mental health or substance use is ‘never a barrier to respective treatment’ (Cambridgeshire and Peterborough CCG et al., 2020).
Our commitment to better care for people with co-occurring Mental Health and Substance/Alcohol use (Cambridgeshire and Peterborough CCG et al., 2020)
The commitment states that delivery of care should be based on the following principles:
- Substance/Alcohol misuse and/or mental health should never be a barrier to respective treatments.
- Dual Diagnosis is a core part of the work of all professionals working in the Mental Health, Substance Misuse and criminal justice field.
- Care should reflect the views and motivations of the person
- Where the person is accessing any combination of substance misuse, mental health and criminal justice services, the service providers will be expected to work collaboratively to meet the needs of the individual through effective joint working and care-coordination arrangements
- Providers will deliver a consistent model of service delivery for those with Dual Diagnosis needs
- Staff of all agencies will be equipped to recognise, assess and support appropriately those with Dual Diagnosis needs
- All staff should have access to relevant training to equip them to manage the care and support of this client group.
- Care plans should involve carers (including young carers) and family members.
- User and carer involvement is at the forefront of service delivery.
- Service providers have responsibility for the delivery of the pathways and should escalate to their commissioner any evidence where the pathway is not being followed
- Where non-compliance of pathway delivery is highlighted, the provider must provide a written action plan to remedy the issues’
Similarly, the Dual Diagnosis and Outreach Team (DDOT) was formed in September 2021, with the aim of removing barriers to care for people who have co-occurring conditions. Service activity data from DDOT has been recorded from November 2021. It has offered an increasing number of contacts over this time, with high rates of attendance (ranging from 88% to 94%).
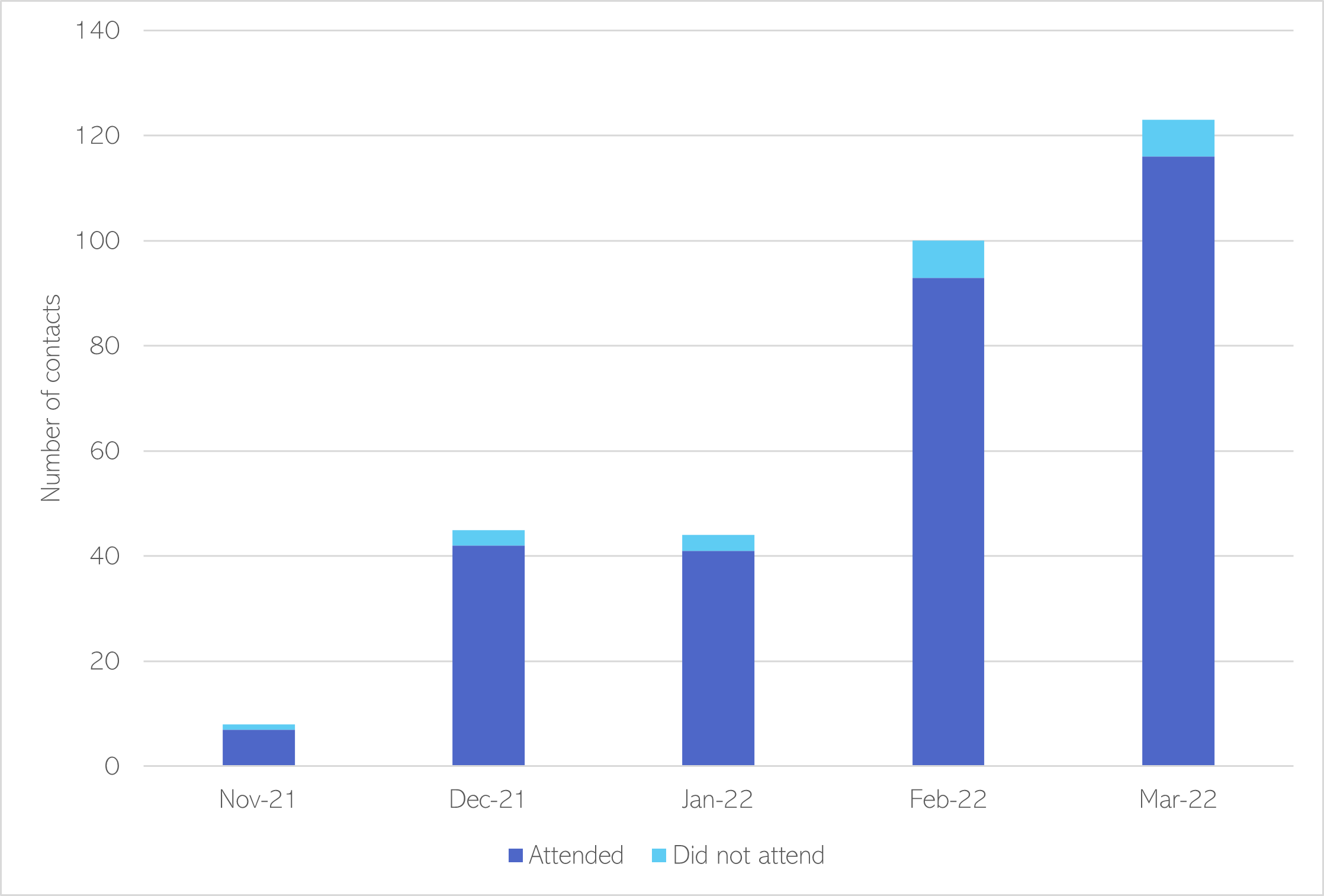
Figure 114: Attendance outcomes in DDOT
What is the local picture: barriers to accessing mental health support?
The 2023 Drugs and Alcohol Needs Assessment (Elvin et al., 2023) highlights that whilst progress has been made in the provision of services, there is a continuing perception that people with co-occurring conditions face significant barriers to accessing mental health support.
- ‘A lack of mental health support and counselling’ was the most commonly given answer by service users asked what was missing from the support they had received from services (Elvin et al., 2023).
- Just 15% of professionals in Cambridgeshire and 10% in Peterborough rated this provision positively, and over half of professional respondents in each area rated it negatively (Elvin et al., 2023).
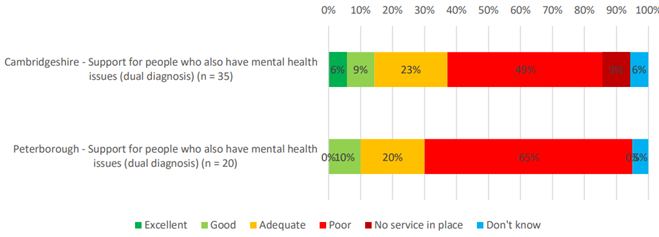
Figure 127: Stakeholder survey respondents’ ratings for support for people who also have mental health issues in Cambridgeshire and Peterborough, Source: (Elvin et al., 2023)
Every interview with professional stakeholders highlighted access to mental health support as a huge problem the in the substance use sector, including how a lack of access can lead to a ‘vicious circle’ of poor mental health and substance use (Elvin et al., 2023).
Local lived experience insights
Local lived experience highlights the importance of understanding why service users may end up missing appointments; and of support workers connecting with individuals at a human level. This work was developed through engagement with the SUN network.
- Stigma and judgement around substance use has a significant impact on people’s lives and ability to engage in services. There is a need for greater understanding, particularly within criminal justice, mental health and housing services.
- Service users deeply appreciate drug and alcohol support workers and mention them by name when feeding back about the service, highlighting the importance of individual connection and compassion.
- Similarly, many service users feel it is important to find a service which is non-judgemental and find it easier to connect with support workers who have lived experience.
- Service users appreciate drop-in sessions, where they can meet other people in recovery and support each other.
- People who have experienced trauma may struggle with change, hence staff turnover can be difficult.
Why do individuals miss appointments?
- Some individuals end up being discharged from services as they may appear ‘unwilling to engage’, but there are many reasons why people may not attend appointments for example because of changes in their life circumstances, such as housing issues; or due to socioeconomic factors, such as being unable to afford transportation to services.
- Another common reason for missing appointments is due to timing: people with substance use may have a limited window of time in which they feel ready and able to engage with services.
- This need to shift focus from ‘people who don’t attend appointments’ to the way appointment systems are managed has been highlighted in previous lived experience work (Centre for Mental Health, 2022a).
Further work on how to ‘transform, democratise and humanise health care’ by expanding opportunities for people with lived experience is detailed in a recent report by the Centre for Mental Health (Centre for Mental Health, 2022a).
Barriers to accessing mental health support
‘Some people’s needs are seen as ‘too complex/ challenging’ for mainstream mental health services, but are not considered acute enough for specialised services. In this way individuals’ access to support is determined by placing the onus on individuals to ‘fit’ the needs of the service, rather than encouraging the system to flex and meet the needs of individuals’ (Making Every Adult Matter, 2022)
A rapid literature review was undertaken for this health needs assessment to better understand different types of barriers to treatment faced by people with co-occurring conditions. These including factors relating to access to, and experiences of, support services.
Access
‘Some people’s needs are seen as ‘too complex/ challenging’ for mainstream mental health services, but are not considered acute enough for specialised services. In this way individuals’ access to support is determined by placing the onus on individuals to ‘fit’ the needs of the service, rather than encouraging the system to flex and meet the needs of individuals’ (Making Every Adult Matter, 2022)
Personal barriers included individual vulnerabilities, beliefs and knowledge and life circumstances and experiences were identified. These barriers can be compounded for people with intellectual or other disabilities, physical health issues, SMI and experience of poverty or based on characteristics such as race, gender, sexuality [(Ledingham et al., 2022),(Priester et al., 2016),(Hawkings & Gilburt, 2017),(Making Every Adult Matter, 2022)].
Individual vulnerabilities
- For some people, the interaction of substance use together with specific mental health diagnoses can lead to individual vulnerabilities, such as decreased motivation and ability to seek and access treatment and affected emotional and cognitive capacity. [(Priester et al., 2016), (Ghouchani et al., 2021),(Ross et al., 2015)].
- A lack of a support system, such as friends and family, is also identified as personal barrier to accessing treatment (Ghouchani et al., 2021).
Individual’s beliefs and knowledge
- An individual’s beliefs can directly impact their accessing treatment. Some people report fear for privacy, or of being forced to take medication and its side effects, or of being detained or having children removed from them as reasons to not seek treatment. Some distrust the services and staff and doubt the efficacy of treatment [(Priester et al., 2016) (Mojtabai et al., 2014) (Ghouchani et al., 2021), (Kawecki & Ebert, 2016), (Hawkings & Gilburt, 2017),(Drake et al., 2001)].
- Cultural attitudes to mental illness and substance use can affect help-seeking behaviour (Priester et al., 2016).
- The perceived stigma around substance use and mental health can result in people not disclosing aspects of their need – for example, some believe the label of ‘comorbidity’ is stigmatising and so don’t disclose either their mental health or substance use [(Priester et al., 2016),(Ledingham et al., 2022), (Ghouchani et al., 2021), (Salameh et al., 2021), (Kawecki & Ebert, 2016), (Hawkings & Gilburt, 2017), (Kelly & Holahan, 2022)].
- A lack of awareness of treatment options and of where to go for support can be a barrier for some [(Ghouchani et al., 2021), (Salameh et al., 2021), (Mojtabai et al., 2014), (Kawecki & Ebert, 2016)].
Individual’s life circumstances and experiences
- An individual’s socioeconomic circumstances can affect their likelihood of seeking treatment. Housing insecurity, poverty, needing to prioritise work and childcare can result in people not considering and prioritising their need for help [(Ghouchani et al., 2021), (Priester et al., 2016), (Ross et al., 2015), (Mojtabai et al., 2014), (Kelly & Holahan, 2022)].
‘It’s the cornerstone of it really – if you don’t have the basics you know, food and shelter – it’s really difficult to feel like you’re in a place where you can have recovery. [But] housing needs to be stable…. because private renters it’s really precarious.’ (Kelly & Holahan, 2022)
- People’s prior experience of care can impact of their willingness to engage with services again.
Poor access to treatment
- It is commonly reported that people with dual diagnosis may be excluded from mental health treatment or treatment is stopped when substance use is known and abstinence is required [(Priester et al., 2016), (Kelly & Holahan, 2022)].
- There appears to be a gap in provision, whereby some individuals present with needs that are ‘too complex or challenging’ for mainstream mental health services but ‘not acute enough’ for specialised services (Making Every Adult Matter, 2022).
- Often, services users are receiving care for either their mental health or substance use but not both (Kawecki & Ebert, 2016).
- Some report a bias towards selecting clients who are likely to have positive outcomes, or referrals being refused if an individual is known and deemed ‘not suitable’ for the service. The way in which services are evaluated and reported may act as a disincentive to treat some individuals (Priester et al., 2016).
- Long waiting times, especially for psychiatry, can act against a ‘small window of opportunity’ for an individual who asks for help [(Ledingham et al., 2022), (Priester et al., 2016), (Ross et al., 2015), (Making Every Adult Matter, 2022)].
- Some services are reported to not be culturally appropriate which can act as a barrier for some individuals [(Priester et al., 2016),(Kawecki & Ebert, 2016)].
‘My religious needs. They’re not recognising things (…) because they come from a different society than what I’ve been brought up in (…).’ (Kawecki & Ebert, 2016).
- A lack of outreach services, or accessible services in rural locations, can be a barrier (Priester et al., 2016).
Experience
Structural factors impact people’s experience of treatment with co-occurring substance use and mental health conditions included poor access, staff training and service quality.
Staff training
- Staff training appears frequently in the literature, with reference to the lack of understanding of substance use in mental health services and vice versa, and the need for better training around managing co-occurring conditions [(Priester et al., 2016), (Kawecki & Ebert, 2016), (Kelly & Holahan, 2022)].
- The consequence of insufficient training is reported to be under-diagnosis (Priester et al., 2016), lack of confidence in discussing substance use with patients and some clinicians reluctant to diagnose substance use if they couldn’t offer any support (Drake et al., 2001).
- The literature cited a lack of trauma-informed approaches which can lead to people being deemed to be ‘untreatable’ or ‘not appropriate’ for the service; this can also be exacerbated by gaps in the service pathway, e.g. for people whose need sits between mainstream mental health support and specialist secondary services (Making Every Adult Matter, 2022).
‘Mental health teams need to be trained in addiction and addiction teams need to be trained in mental health – there has to be an understanding there. You don’t have to know how to fix it, but you have to know where to go to get help. You have to have an understanding about how that affects the person and what they do.’ – Amy, Substance Use Disorder/Alcohol Use Disorder led NGO (Kelly & Holahan, 2022)
Quality of services
- Factors relating to the quality of services were identified as barriers. This included understaffing, short appointment lengths and high staff turnover [(Ross et al., 2015),(Kawecki & Ebert, 2016),(Making Every Adult Matter, 2022)]. A lack of continuity in care can promote apathy and distrust form service users.
‘I ain’t got nothing to talk about when I ain’t going to see them next month. When they’re going to be gone and I’m going to be assigned another case manager.’ (Kawecki & Ebert, 2016)
- A lack of communication and collaboration between providers can result in over or under referrals, and uncoordinated support which can engender a sense of apathy in service users. Sometimes this is driven by funding mechanisms leading to fragmentation of delivery and poor coordination of care [(Ross et al., 2015), (Kawecki & Ebert, 2016),(Kelly & Holahan, 2022), (Making Every Adult Matter, 2022)].
‘If somebody is in homeless services, they can’t access community mental health services, because they’re homeless. And with no disrespect to the homeless mental health teams, it can sometimes be difficult to get the client assessed.’ – Philip, Housing led NGO (Kelly & Holahan, 2022)
- Narrowly defined outcome measures can act as disincentives to support people with co-occurring conditions (Making Every Adult Matter, 2022).
- A ‘traditional’ service offer that is not flexible towards the particular needs of people with co-occurring conditions can become a barrier to accessing treatment e.g. multiple missed appointments leading to someone being discharged from the service [(Priester et al., 2016), (Kawecki & Ebert, 2016), (Making Every Adult Matter, 2022)]. Another example is the IAPT aim to get people through treatment within 6 or 12 weeks, which may not be enough time for patients with more complex needs (405).
- Service users may be refused treatment due to the complexity of their need or their behaviour, rather than due to their substance use, with practitioners citing that the therapies on offer don’t meet the level of need of the individual (Making Every Adult Matter, 2022).
- The literature documented how staff’s personal values may sometimes reinforce and drive stigma and discrimination; a lack of empathy or respect may result in individuals with co-occurring conditions not disclosing their needs. Sometimes staff’s perception of a diagnosis may result in them not identifying a need; one example provided in the literature was of clinicians diagnosing adolescents with psychiatric conditions rather than substance use for fear they would be stigmatised [(Ghouchani et al., 2021), (Priester et al., 2016), (Ross et al., 2015), (Kawecki & Ebert, 2016)].
‘[The service user] perceived that her appearance, her mental history, and alcohol addiction contributed to difficulties in obtaining adequate diagnosis and care for her health. (…) Repeatedly, [her] clinical presentation led her to be treated as if she were psychotic when, in fact, she was in severe withdrawal with and delirium tremens.’ (Villena & Chesla, 2010)
Facilitators to accessing mental health support
3 categories of facilitators to people with co-occurring conditions accessing support were identified from the review of the literature:
- Reviewing specialist knowledge and approaches within mental health, substance use and primary care
- Supporting a more integrated approach with continuity of care
- Supporting people to enable more effective treatment.
Review specialist knowledge and approaches within mental health, substance use and primary care
- Increase knowledge around co-occurring conditions across teams: mental health, substance use and primary care services all need to recognise and manage the interdependence of mental health conditions and substance use [(Priester et al., 2016), (Making Every Adult Matter, 2022), (Ledingham et al., 2022), (Public Health England, 2017)].
- Education and training: to support understanding of substance use and tackle myths within mental health settings and vice versa, and to promote appropriate referrals (Elvin et al., 2023).
- Address multiple disadvantage: increase mental health services’ understanding and ability to work in partnership to address the experiences of people facing multiple disadvantage experience e.g. substance use, housing issues, poverty and trauma (Making Every Adult Matter, 2022).
- New pathways: consider developing new pathways, such as a ‘complex needs service’ for personality disorders and complex trauma, offering psychologically informed care which does not exclude substance users (Elvin et al., 2023).
- Longer term approaches: long-term support may be needed for some individuals [NHS England, 2016].
- Outreach, peer support and rapid access: more assertive outreach support (Ward, 2016), peer support [(Kawecki & Ebert, 2016), (Ledingham et al., 2022)] and enabling quick access to support when needed [(Kawecki & Ebert, 2016), (Making Every Adult Matter, 2022)].
Support a more integrated approach with continuity of care
- Joint commissioning and protocols: clearer joint working agreements, information-sharing, protocols, and procedures for co-occurring conditions pathway [(Elvin et al., 2023), (Public Health England, 2017), (Kawecki & Ebert, 2016)].
- Use existing enablers: embed existing mechanisms, such as warm handovers.
- Transparent pathways: have a clear service map that includes how decisions are made, in terms of who is accepted for treatment and review service access criteria with experts by experience (Public Health England, 2017).
- Monitoring and incentives: monitor providers on effectiveness of response to particular groups and consider incentivising contracts to support engagement and positive outcomes for people with additional vulnerability factors (Public Health England, 2017).
- Holistic outcome measures: ensure incentives align to treat people with co-occurring conditions to avoid cherry-picking or people deemed to be ‘unsuitable’ [(Making Every Adult Matter, 2022), (Priester et al., 2016)].
- Co-location of some services: provide some mental health support in same location as substance use support (Delgadillo et al., 2015).
Supporting people to engage with more effective treatment
- Empowering people: provide information to help people living with co-occurring conditions to understand the impact of treatment to encourage take up when offered [(Ghouchani et al., 2021),(Drake et al., 2001)].
- Flexible support: appointment reminders; more out of hours appointments; revised approach to missed appointments [(Ross et al., 2015), (Priester et al., 2016), (Making Every Adult Matter, 2022), (Kawecki & Ebert, 2016), NICE Guidance 2016, (Public Health England, 2017), (Elvin et al., 2023)].
- Caring for the whole person not the diagnosis: care needs being addressed simultaneously not in siloes including practical help with housing and employment, and support in accessing a wide range of services [(Kawecki & Ebert, 2016), (Kawecki & Ebert, 2016)].
- Supporting positive relationships with staff: enable positive and consistent relationships between service users and staff (with empathy, respect, persistence and perseverance) [(Kawecki & Ebert, 2016), (Kawecki & Ebert, 2016)].
Example: Cambridgeshire Adolescent Substance Use Service
Cambridgeshire Adolescent Substance Use Service (CASUS) is a service for children and young people (up to the age of 18, or age 21 for the most vulnerable young people) provides integrated care for those with co-occurring conditions and may provide an example of a way to avoid many of the barriers listed above.
- CASUS uses the AMBIT integrative measure (AIM) that takes a ‘wide angle’ approach to accessing co-occurring and intersecting needs over 7 different domains. This aims to ‘legitimise focus on other issues alongside the substance misuse itself’.
- CASUS uses adaptive mentalisation based integrative treatment (AMBIT), a treatment approach for people with multiple complex needs, which focuses on responding to what a young person sees as helpful to them in order to engage them in support services (Fuggle et al., 2021).
- From AMBIT, a range of evidence-based interventions are used to support young people, including CBT for anxiety and motivational interviewing.
- Multi-agency collaboration, such as with housing and youth offending services, is central to this.
- An evaluation of CASUS from 2013 to 2017 found (Fuggle et al., 2021):
- Significant reductions in cannabis and alcohol use.
- Functional improvements in 5 out of 7 domains.
- It suggests CASUS achieved ‘substantial improvements in many areas of life functioning such as family and peer relationships, education and mental health for individual young people as part of the treatment for substance use’.
Additional resources
- The local data pack gives an overview of key data and trends
- NICE guidelines Coexisting severe mental illness and substance misuse: community health and social care services
- Turning Point’s Dual Diagnosis toolkit
- A literature review of dual diagnosis
- An overview of trauma and trauma-informed care
- The experiences of local service users, told in their own words
- Facilitators and barriers in dual recovery: A literature review of first-person perspectives
References
Full list of references is included at the end of this chapter.