Local stakeholder survey
In October 2024, a local stakeholder survey (targeted at services that support individuals who self-harm or attempt suicide) was conducted as part of this needs assessment via Microsoft Forms. The survey aimed to identify strengths and gaps in current services.
- The survey received 120 responses from more than nine sectors across Cambridgeshire and Peterborough, with the majority coming from Health (58%) (mainly CPFT) and Education (23%) (predominantly schools) (Figure 42).
- It is important to note that this was not a representative sample, as stakeholders who are more knowledgeable or have strong opinions may have been more likely to complete the survey.
- The survey included both rating and free-text questions. Free-text responses were analysed thematically, with each response reviewed for recurring themes. The most common themes are summarised below, along with representative quotes.

Figure 42: Survey responses by organisation
Stakeholders were asked to rate various aspects of the current system supporting people who self-harm and attempt suicide (Figure 43 and 44). For both self-harm and suicide, the most positively rated aspects were clarity where to signpost and support after crisis (majority rated these as fair or better). However, coordination between providers and support and involvement of family/carers were rated poorly (over 50% rated support for families/carers as poor or very poor for self-harm and around 45% for attempted suicide).
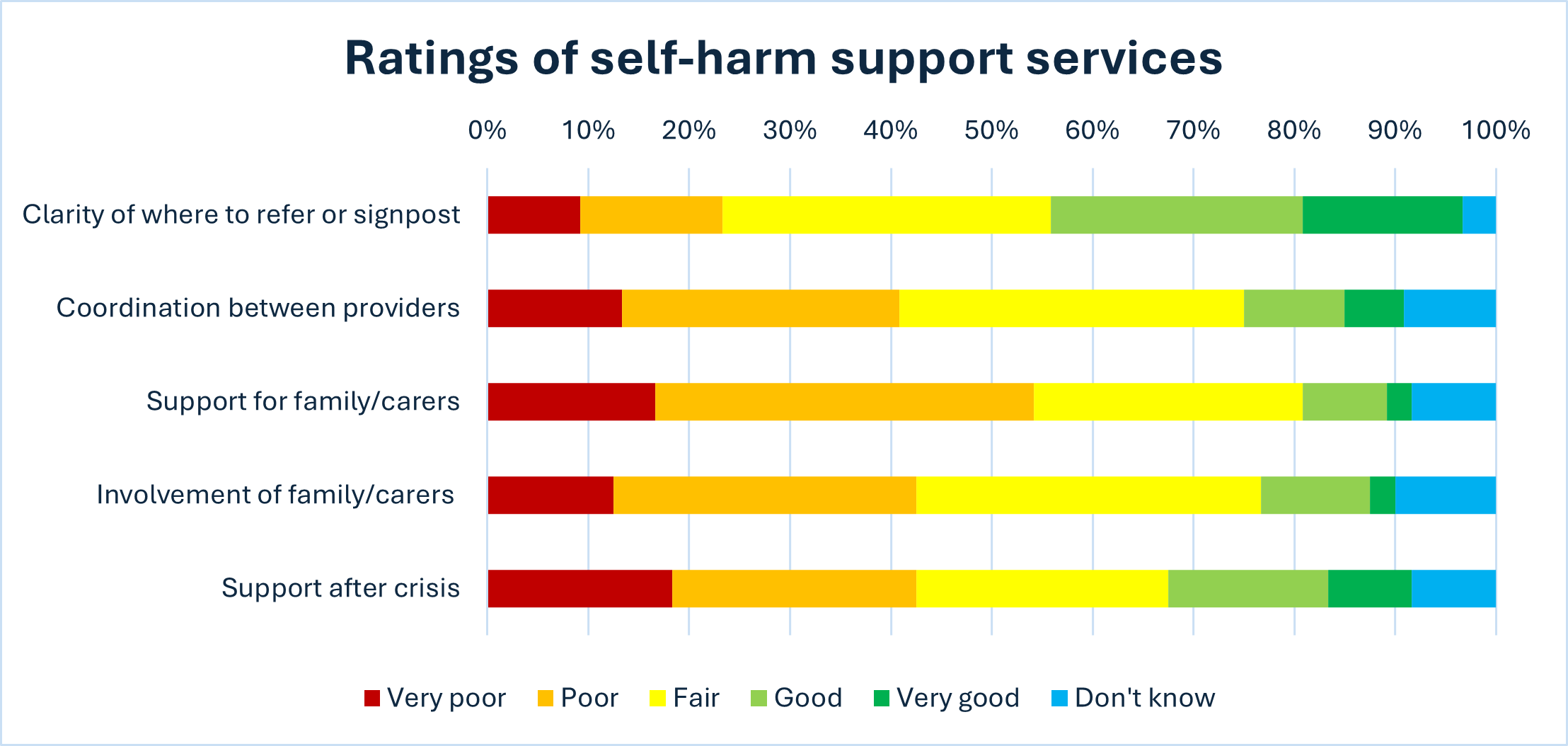
Figure 43: Ratings of Self-harm Support Services
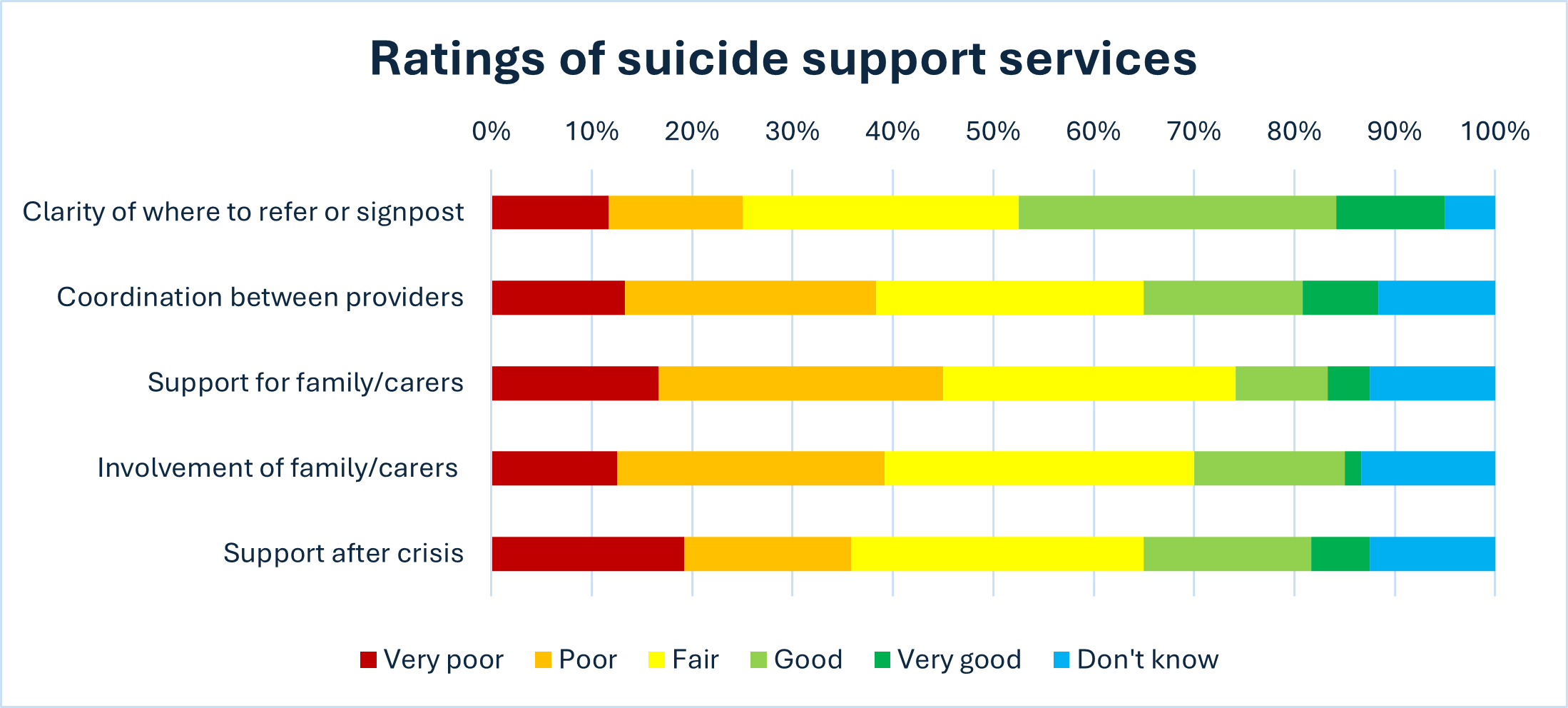
Figure 44: Ratings of Suicide Attempt Support Services
Responses by service type
When comparing responses from the two main responding organisations – CPFT and Education – responses from Education representatives tended to be more negative, with some respondents stating that are no or limited strengths in the system supporting people who self-harm or have attempted suicide. Others mentioned that support within their school was a strength. The main gaps raised by education staff was an overall lack of support for young people who self-harm or attempt suicide. This included a lack of early intervention, as well as a lack of post-crisis support. People also reported issues could arise due to poor coordination between health services and schools. These seem to reflect Fullscope’s research findings that teaching staff feel ill-equipped to have the difficult conversation about self-harm with pupils and feeling nervous for fear of making the situation worse.
Self-harm support – strengths and gaps
For self-harm support, respondents listed several strengths, including effective multi-agency collaboration, the 111 option 2 for mental health crises, and strong individual team efforts. Specific services praised included crisis services, CPFT community mental health services, voluntary and community sector organisations, and support in schools. The Personality Disorder Community Service (PDCS and REDS) stood out as the most commonly praised service. However, many noted limitations, citing capacity issues, funding constraints, and staff shortages that often hinder support efforts. Other respondents felt that there are no strengths.
‘I have found that FRS has been very effective for some people in de-escalating distress when they’re in crisis’
‘I have found REDS service very helpful with their online self directed course. It really helps to bridge the gap with the wait for in person support.’
‘No strengths, it’s a broken system that often leads to patients feeling worse.’
‘There are some very good professionals about, but they are very stretched which is a barrier to them providing effective support.’
The main gaps identified were long waiting times for community mental health and crisis support, and insufficient early intervention. Respondents expressed concerns over limited support for families, specific vulnerable groups (including people under the influence of drugs/alcohol, neurodivergent people, learning disabled people, those in some geographic areas), and post-crisis follow-up.
Whilst some people mentioned coordination as a strength, other people highlighted a lack coordination across services as a key gap, including issues with communication and data sharing between all the different organisations involved in someone’s care. Some also noted a lack of awareness and training on self-harm support options.
‘It feels that currently all services are stretched and therefore waiting lists are long and intervention and support is brief and not thorough. We need to be looking at prevention work instead of firefighting with a water gun.’
‘Often have found family have identified there is an issue and try to get help but no help is offered until it’s at crisis point and by then a lot of damage is done and hard to undo.’
Support after a suicide attempt – strengths and gaps
Similar strengths were noted in support for individuals who have attempted suicide as for those who self-harm. Many respondents raised good system coordination and specific teams, particularly CPFT crisis teams, the Crisis Resolution and Home Treatment Team (CRHTT), and the First Response Service/111. However, like with self-harm support, a significant number felt there were few strengths in the current system, citing underfunding, siloed structures, and poor inter-team communication as ongoing challenges despite staff efforts.
‘Effective team working and fast lines of communication have been effective in responding to these situations and reducing a number of completions’
‘There are a lot of skilled and dedicated people trying to do their best in a complex, under resourced system that is need of major reform.’
Key gaps mentioned included a lack of ongoing support post-crisis, long waiting times, and high thresholds for accessing services. Respondents also highlighted issues with funding, staffing, and workload, which restrict service effectiveness. Many people felt that people who have attempted suicide could have very negative experiences of mental health services. They raised specific concerns around a lack of support for young people, and the family or carers of people who have attempted suicide.
‘…support is far better immediately after an episode that involves attempted suicide than later on. Sometimes, this feels like patching-up a significant problem rather than managing the underlying cause.’
‘There is no on-going help. They get seen at A&E or the 136 suite, and are discharged from there. … if they feel low again have to start the whole process from the beginning again.’
Awareness of suicide prevention offers
Awareness of suicide prevention services was generally low, with the exception of Samaritans (98% awareness) (Figure 45). A significant proportion of respondents were unaware of services such as ‘Ask Me How I Am’ (75% unaware), Lifecraft’s bereavement support (58% unaware), Lifeline (46% unaware), and STOP Suicide training (46% unaware). Increasing awareness of these services across organisations is a clear recommendation.

Figure 45: Awareness of Suicide Prevention offers
Other resources and training that respondents had found helpful are summarised in Table 9.

Table 9: Suicide Prevention Resources Found Helpful by Respondents